

The combination of gene hyperamplification and PD-L1 expression as a biomarker for the clinical benefit of tislelizumab in gastric/gastroesophageal junction adenocarcinoma
- PMID: 35778636
- PMCID: PMC9365737
- DOI: 10.1007/s10120-022-01308-7
The combination of gene hyperamplification and PD-L1 expression as a biomarker for the clinical benefit of tislelizumab in gastric/gastroesophageal junction adenocarcinoma
Abstract
Background: In solid tumor Phase 1/2 trials (NCT02407990; NCT04068519), tislelizumab demonstrated clinical benefit, including in advanced gastroesophageal adenocarcinoma (GEA). However, the majority of patients with GEA did not respond, highlighting the need to understand mechanisms of resistance and identify predictive biomarkers for response.
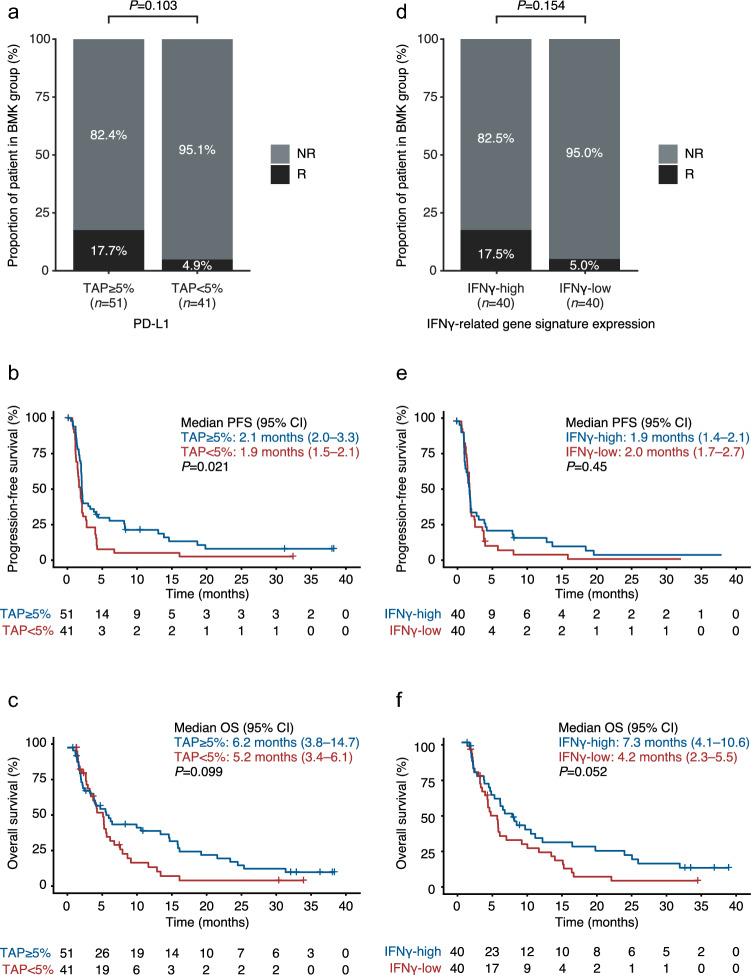
Methods: All tislelizumab-treated patients with GEA from the Phase 1/2 trials were included (N = 105). Programmed death-ligand 1 (PD-L1) expression (Tumor Area Positivity [TAP] ≥ 5%), interferon gamma (IFNγ)-related gene signature, gene expression profile, tumor mutational burden (TMB), and gene hyperamplification (HA) were analyzed for correlation with tislelizumab.
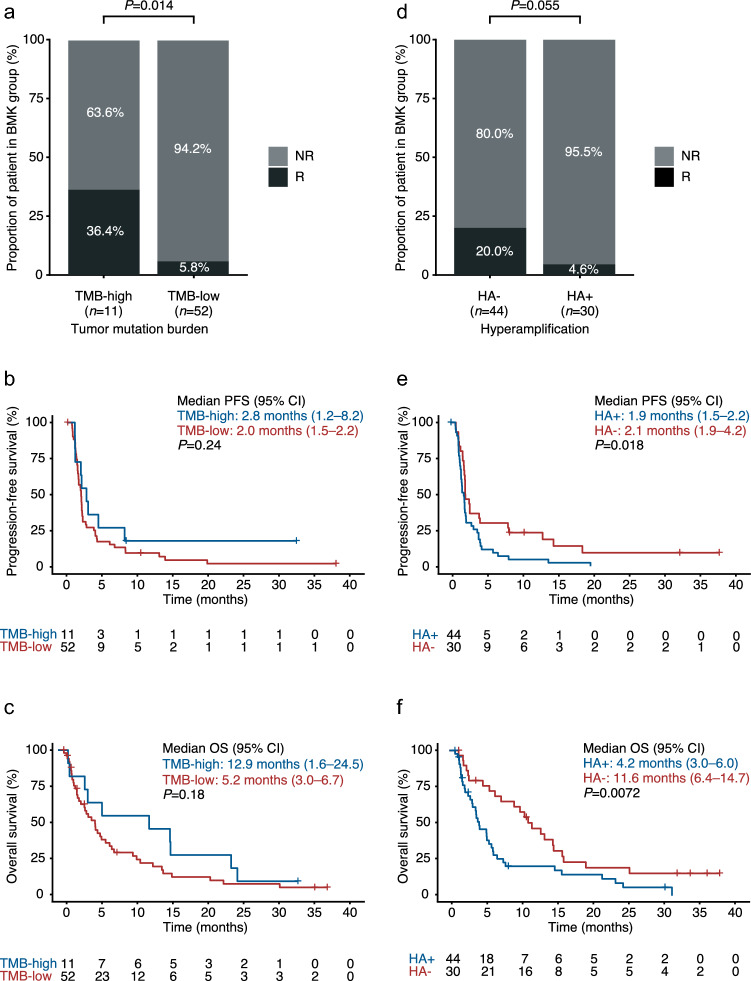
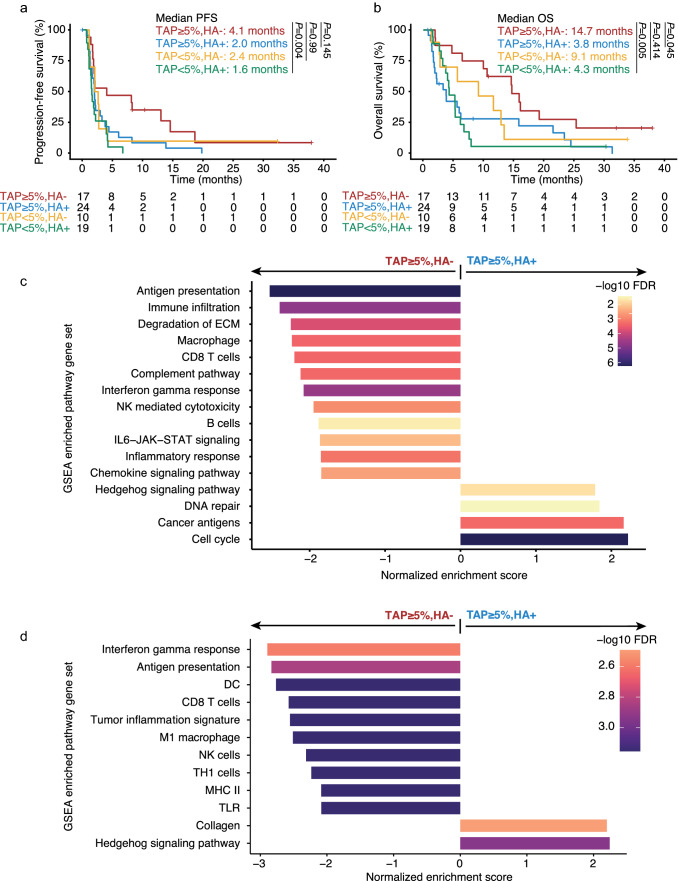
Results: A moderate association was observed between PD-L1 TAP ≥ 5%, IFNγ gene signature, TMB-high and efficacy. A potential correlation between hyperamplification (HA +) and worse outcomes with programmed cell death protein 1 (PD-1) inhibition was identified. Hyperamplified genes were mainly enriched in cancer progression pathways, including cell cycle and RTK-RAS-PI3K pathways. Joint PD-L1 TAP ≥ 5% and lack of hyperamplification showed the most favorable benefit with an objective response rate of 29.4%, and median progression-free survival and overall survival of 4.1 and 14.7 months, respectively. Tumors with TAP ≥ 5% and HA - had inflamed immune signatures with increased immune cell infiltration, enhanced anti-tumor cytotoxic activity and antigen presentation signatures. Findings were validated in two independent gastric and gastrointestinal cancer cohorts treated with immune checkpoint inhibitors.
Conclusions: In GEA, PD-L1 positivity, IFNγ-related gene signature and TMB-high status were positively associated with tislelizumab clinical benefit, whereas HA was associated with worse clinical outcomes. Combining PD-L1 positivity and HA - may help identify patients more likely to benefit from PD-1 blockade.
Keywords: Gastroesophageal adenocarcinoma; Hyperamplification; Immuno-oncology; PD-(L)1 inhibitor; PD-L1.
© 2022. The Author(s).
Conflict of interest statement
S. Yang, X. Luo, Y. Shi, Y. Zhang, R. Huang, Y. Xu and Z. Shen are employees of BeiGene and hold BeiGene stock. Z. Lu, JS. Lee, S. Deva, T. Liu, Y. Chao, and L. Shen report no conflicts of interest.
Figures

References
-
- Fashoyin-Aje L, Donoghue M, Chen H, He K, Veeraraghavan J, Goldberg KB, et al. FDA approval summary: pembrolizumab for recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma expressing PD-L1. Oncologist. 2019;24(1):103–109. doi: 10.1634/theoncologist.2018-0221. - DOI - PMC - PubMed
-
- Kang YK, Boku N, Satoh T, Ryu MH, Chao Y, Kato K, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;390(10111):2461–2471. doi: 10.1016/S0140-6736(17)31827-5. - DOI - PubMed
-
- Shitara K, Özgüroğlu M, Bang YJ, Di Bartolomeo M, Mandalà M, Ryu MH, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. 2018;392(10142):123–133. doi: 10.1016/S0140-6736(18)31257-1. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
