

Single-isocenter multiple-target stereotactic radiosurgery for multiple brain metastases: dosimetric evaluation of two automated treatment planning systems
- PMID: 35778741
- PMCID: PMC9250172
- DOI: 10.1186/s13014-022-02086-3
Single-isocenter multiple-target stereotactic radiosurgery for multiple brain metastases: dosimetric evaluation of two automated treatment planning systems
Abstract
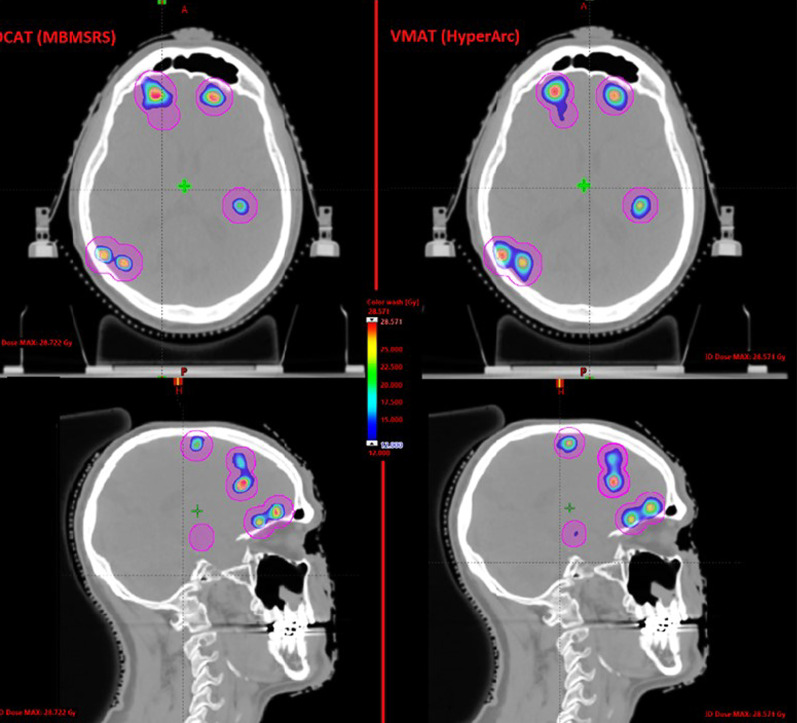
Purpose: Automated treatment planning systems are available for linear accelerator (linac)-based single-isocenter multi-target (SIMT) stereotactic radiosurgery (SRS) of brain metastases. In this study, we compared plan quality between Brainlab Elements Multiple Brain Metastases (Elements MBM) software which utilizes dynamic conformal arc therapy (DCAT) and Varian HyperArc (HA) software using a volumetric modulated arc therapy (VMAT) technique.
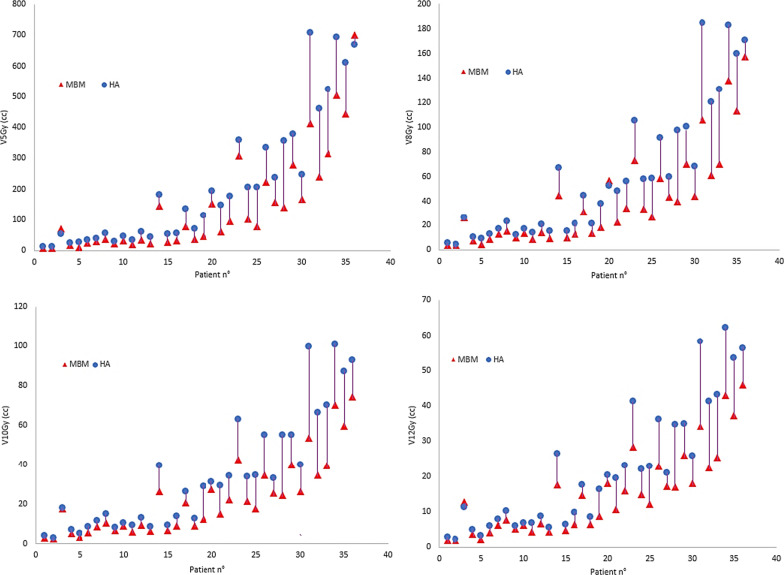
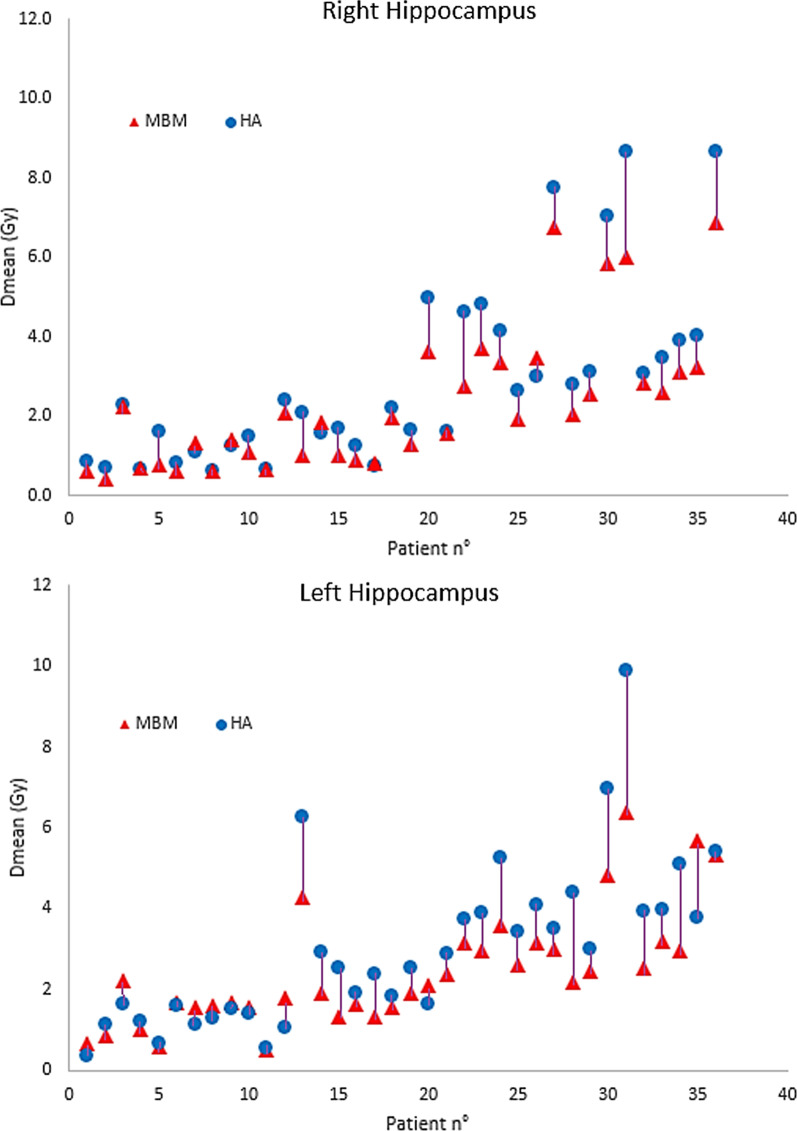
Patients and methods: Between July 2018 and April 2021, 36 consecutive patients ≥ 18 years old with 367 metastases who received SIMT SRS at UPMC Hillman Cancer San Pietro Hospital, Rome, were retrospectively evaluated. SRS plans were created using the commercial software Elements MBM SRS (Version 1.5 and 2.0). Median cumulative gross tumor volume (GTV) and planning tumor volume (PTV) were 1.33 cm3 and 3.42 cm3, respectively. All patients were replanned using HA automated software. Extracted dosimetric parameters included mean dose (Dmean) to the healthy brain, volumes of the healthy brain receiving more than 5, 8,10, and 12 Gy (V5Gy, V8Gy, V10Gy and V12Gy), and doses to hippocampi.
Results: Both techniques resulted in high-quality treatment plans, although Element MBM DCAT plans performed significantly better than HA VMAT plans, especially in cases of more than 10 lesions). Median V12Gy was 13.6 (range, 1.87-45.9) cm3 for DCAT plans and 18.5 (2.2-62,3) cm3 for VMAT plans (p < 0.0001), respectively. Similarly, V10Gy, V8Gy, V5Gy (p < 0.0001) and median dose to the normal brain (p = 0.0001) were favorable for DCAT plans.
Conclusions: Both Elements MBM and HA systems were able to generate high-quality plans in patients with up to 25 brain metastases. DCAT plans performed better in terms of normal brain sparing, especially in patients with more than ten lesions and limited total tumor volume.
Keywords: Brain metastases; DCAT; Single-isocenter multiple-targets radiosurgery; Stereotactic radiosurgery; VMAT.
© 2022. The Author(s).
Conflict of interest statement
GM received speaker honoraria from Brainlab. The other authors declare that they have no competing interests.
Figures
References
-
- Kocher M, Soffietti R, Abacioglu U, Villà S, Fauchon F, Baumert BG, Fariselli L, Tzuk-Shina T, Kortmann RD, Carrie C, Hassel MB, Kouri M, Valeinis E, van den Berge D, Collette S, Collette L, Mueller RP. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952–26001 study. J Clin Oncol. 2011;29:134–141. doi: 10.1200/JCO.2010.30.1655. - DOI - PMC - PubMed
-
- Brown PD, Jaeckle K, Ballman KV, Farace E, Cerhan JH, Anderson SK, Carrero XW, Barker FG, 2nd, Deming R, Burri SH, Ménard C, Chung C, Stieber VW, Pollock BE, Galanis E, Buckner JC, Asher AL. Effect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trial. JAMA. 2016;316(4):401–409. doi: 10.1001/jama.2016.9839. - DOI - PMC - PubMed
-
- Grandhi R, Kondziolka D, Panczykowski D, Monaco EA, 3rd, Kano H, Niranjan A, Flickinger JC, Lunsford LD. Stereotactic radiosurgery using the Leksell Gamma Knife Perfexion unit in the management of patients with 10 or more brain metastases. J Neurosurg. 2012;117(2):237–245. doi: 10.3171/2012.4.JNS11870. - DOI - PubMed
-
- Yamamoto M, Serizawa T, Shuto T, Akabane A, Higuchi Y, Kawagishi J, Yamanaka K, Sato Y, Jokura H, Yomo S, Nagano O, Kenai H, Moriki A, Suzuki S, Kida Y, Iwai Y, Hayashi M, Onishi H, Gondo M, Sato M, Akimitsu T, Kubo K, Kikuchi Y, Shibasaki T, Goto T, Takanashi M, Mori Y, Takakura K, Saeki N, Kunieda E, Aoyama H, Momoshima S, Tsuchiya K. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014;15(4):387–395. doi: 10.1016/S1470-2045(14)70061-0. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
