

A Case of Methicillin-Sensitive Staphylococcus aureus (MSSA) Prostate Abscess, Osteomyelitis, and Myositis Associated with MSSA Bacteremia in a 60-Year-Old Patient Presenting with Back Pain
- PMID: 35778821
- PMCID: PMC9257711
- DOI: 10.12659/AJCR.936704
A Case of Methicillin-Sensitive Staphylococcus aureus (MSSA) Prostate Abscess, Osteomyelitis, and Myositis Associated with MSSA Bacteremia in a 60-Year-Old Patient Presenting with Back Pain
Abstract
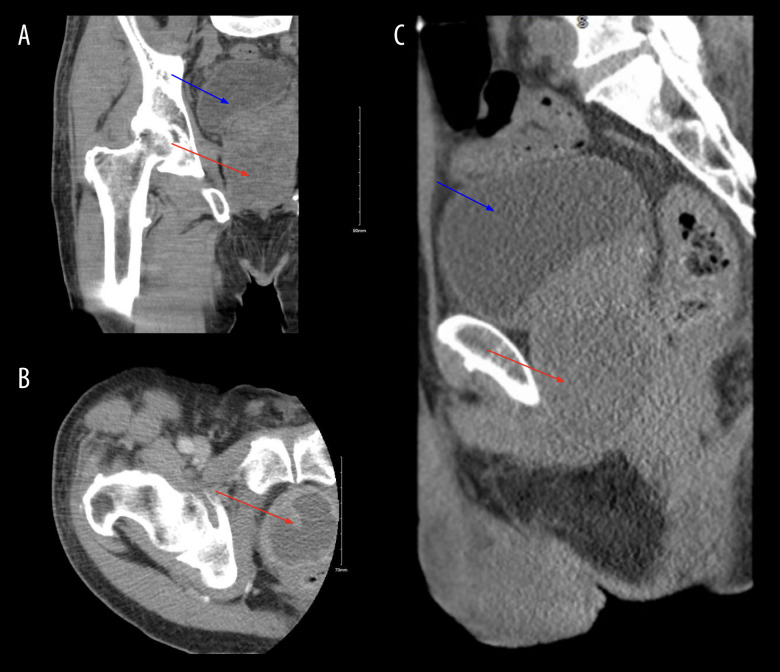
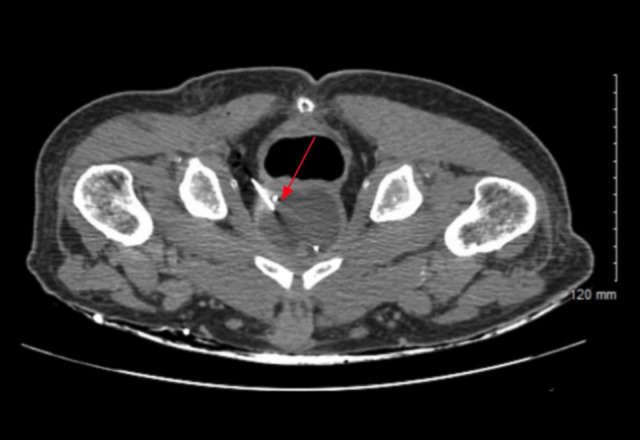
BACKGROUND Staphylococcus aureus (SA) is a rare cause of prostatic abscess. Risk factors include genito-urinary instrumentalization and immunocompromised states. Because of the lack of guidelines on the diagnosis, management, and follow-up of SA prostate abscess, the diagnosis can sometimes be challenging. Our patient was a 60-year-old man who initially presented with lower back pain and was diagnosed with a methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia, prostate abscess, osteomyelitis, and myositis. CASE REPORT A 60-year-old man presented with lower back pain. He had a past medical history of incompletely treated MSSA cervical osteomyelitis with epidural abscess, alcohol use disorder, intravenous drug use (IVDU), and poorly controlled diabetes mellitus (DM). He was afebrile and hemodynamically stable. Laboratory test results revealed leukocytosis and an elevated C reactive protein (CRP). Lumbar spine magnetic resonance imaging (MRI) showed vertebral osteomyelitis and right psoas myositis. Blood cultures isolated MSSA. The patient was treated with vancomycin and piperacillin-tazobactam. On day 5, our patient reported having fever, chills, flank pain, and dysuria. Computed tomography (CT) revealed a 4.0×4.9 cm prostatic abscess. CT-guided percutaneous abscess drainage was performed, and fluid culture revealed MSSA. Both antibiotics were discontinued and cefazolin was started following sensitivities. Post-drainage pelvic ultrasound (US) showed resolution of the abscess. CONCLUSIONS This case highlights the importance of a rapid diagnosis of SA prostate abscess in patients with documented risk factors and characteristic symptoms. Timely management with antibiotics and drainage as indicated are imperative to avoid further complications from the underlying bacteremia, including sepsis and metastatic infections.
Conflict of interest statement
Figures

Similar articles
-
Rare cause of back pain: Staphylococcus aureus vertebral osteomyelitis complicated by recurrent epidural abscess and severe sepsis.BMJ Case Rep. 2016 Dec 13;2016:bcr2016217111. doi: 10.1136/bcr-2016-217111. BMJ Case Rep. 2016. PMID: 27965310 Free PMC article.
-
Intracardiac Abscess and Pacemaker Lead Infection Secondary to Hematogenous Dissemination of Methicillin-Sensitive Staphylococcus Aureus from a Prior Diabetic Foot Ulcer and Osteomyelitis.Am J Case Rep. 2018 Mar 1;19:224-228. doi: 10.12659/ajcr.906227. Am J Case Rep. 2018. PMID: 29491344 Free PMC article.
-
Lumbosacral spondylodiscitis complicated by sepsis, osteomyelitis, epidural abscess formation and deep vein thrombosis.BMJ Case Rep. 2020 Dec 28;13(12):e238522. doi: 10.1136/bcr-2020-238522. BMJ Case Rep. 2020. PMID: 33372019 Free PMC article.
-
A case report of iliopsoas abscess and literature review.Medicine (Baltimore). 2024 Aug 16;103(33):e39356. doi: 10.1097/MD.0000000000039356. Medicine (Baltimore). 2024. PMID: 39151535 Free PMC article. Review.
-
Staphylococcus aureus Prostatic abscess: a clinical case report and a review of the literature.BMC Infect Dis. 2017 Jul 21;17(1):509. doi: 10.1186/s12879-017-2605-4. BMC Infect Dis. 2017. PMID: 28732492 Free PMC article. Review.
References
-
- Weinberger M, Cytron S, Servadio C, et al. Prostatic abscess in the antibiotic era. Rev Infect Dis. 1988;10(2):239–49. - PubMed
-
- Granados EA, Riley G, Salvador J, Vincente J. Prostatic abscess: Diagnosis and treatment. J Urol. 1992;148(1):80–82. - PubMed
-
- Barozzi L, Pavlica P, Menchi I, et al. Prostatic abscess: Diagnosis and treatment. Am J Roentgenol. 1998;170(3):753–57. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
