

Construction and validation of a prognostic model based on 11 lymph node metastasis-related genes for overall survival in endometrial cancer
- PMID: 35778922
- PMCID: PMC9741985
- DOI: 10.1002/cam4.4844
Construction and validation of a prognostic model based on 11 lymph node metastasis-related genes for overall survival in endometrial cancer
Abstract
Background: Endometrial cancer (EC) is one of the most common malignant tumors in female reproductive system. The incidence of lymph node metastasis (LNM) is only about 10% in clinically suspected early-stage EC patients. Discovering prognostic models and effective biomarkers for early diagnosis is important to reduce the mortality rate.
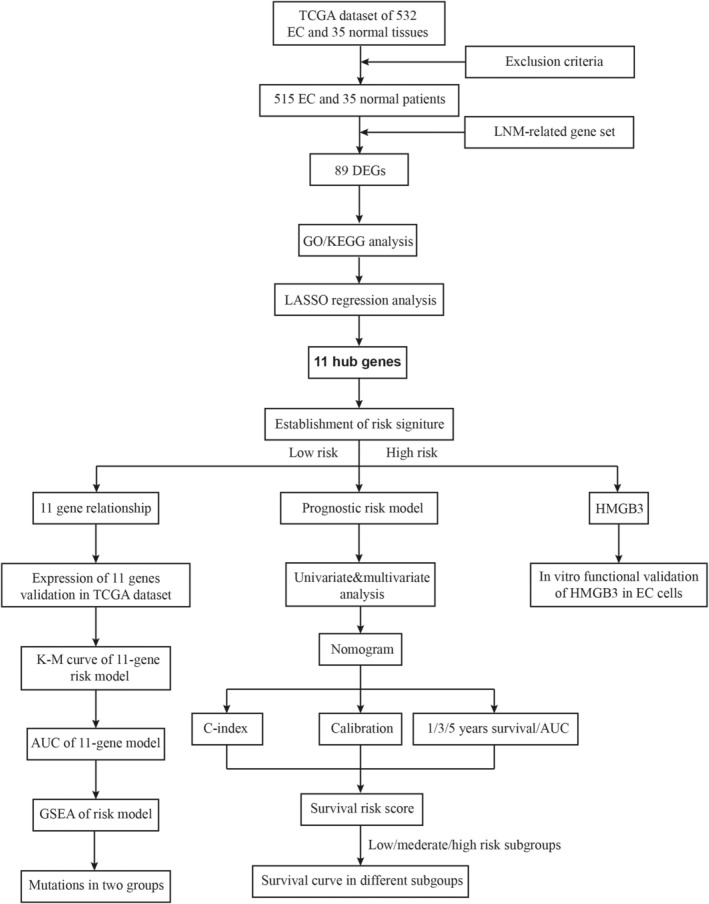
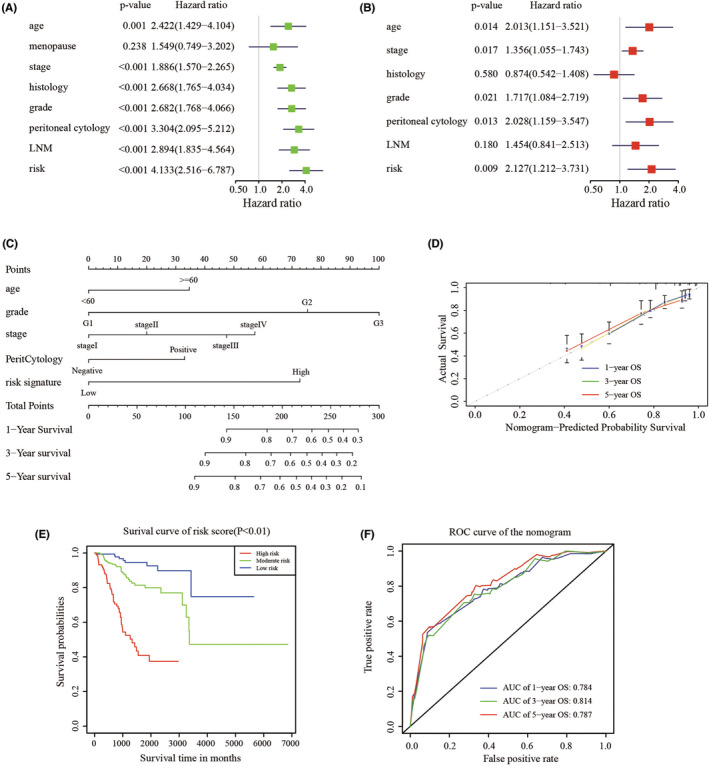
Methods: A least absolute shrinkage and selection operator (LASSO) regression was conducted to identify the characteristic dimension decrease and distinguish porgnostic LNM related genes signature. Subsequently, a novel prognosis-related nomogram was constructed to predict overall survival (OS). Survival analysis was carried out to explore the individual prognostic significance of the risk model and key gene was validated in vitro.
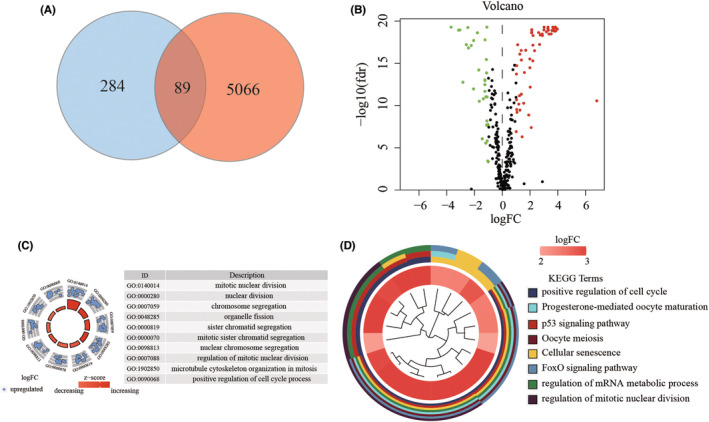
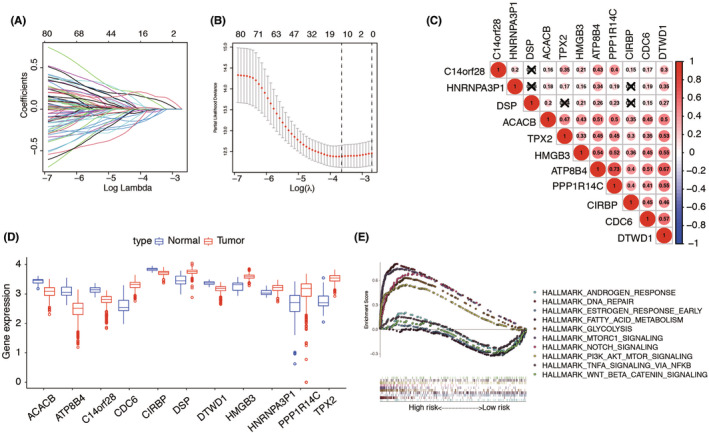
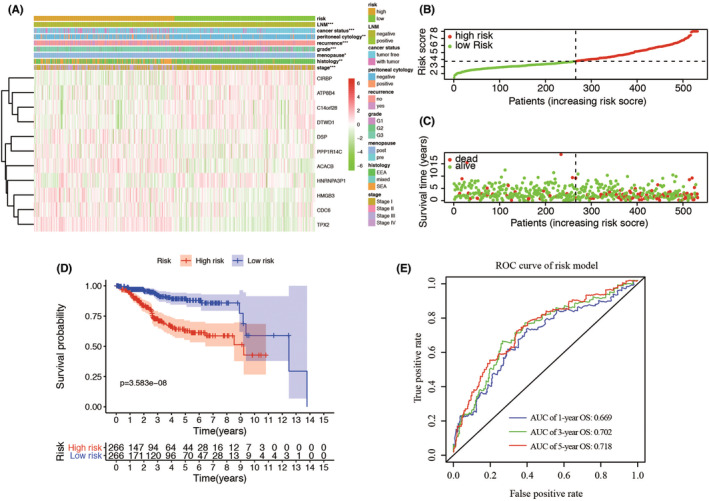
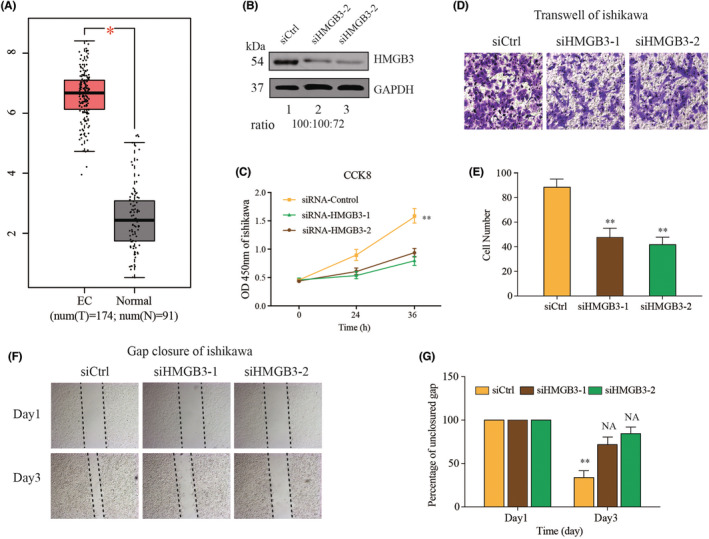
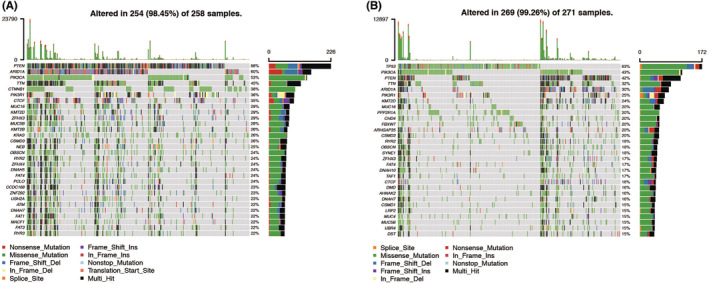
Results: In total, 89 lymph node related genes (LRGs) were identified. Based on the LASSO Cox regression, 11 genes were selected for the development of a risk evaluation model. The Kaplan-Meier curve indicated that patients in the low-risk group had considerably better OS (p = 3.583e-08). The area under the ROC curve (AUC) of this model was 0.718 at 5 years of OS. Then, we developed an OS-associated nomogram that included the risk score and clinicopathological features. The concordance index of the nomogram was 0.769. The survival verification performed in three subgroups from the nomogram demonstrated the validity of the model. The AUC of the nomogram was 0.787 at 5 years OS. Proliferation and metastasis of HMGB3 were explored in EC cell line. External validation with 30 patients in our hospital showed that patients with low-risk scores had a longer OS (p-value = 0.03). Finally, we revealed that the most frequently mutated genes in the low-risk and high-risk groups are PTEN and TP53, respectively.
Conclusions: Our results suggest that LNM plays an important role in the prognosis, and HMGB3 was potential as a biomarker for EC patients.
Keywords: HMGB3; endometrial cancer; lymph node metastasis; mutation; risk signature.
© 2022 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7‐30. - PubMed
-
- Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115‐132. - PubMed
-
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet. 2009;105:103‐104. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
