Risk of hospitalization and death for COVID-19 in persons with epilepsy over a 20-month period: The EpiLink Bologna cohort, Italy
- PMID: 35778963
- PMCID: PMC9349826
- DOI: 10.1111/epi.17356
Risk of hospitalization and death for COVID-19 in persons with epilepsy over a 20-month period: The EpiLink Bologna cohort, Italy
Abstract
Objective: Data on COVID-19 outcomes in persons with epilepsy (PWE) are scarce and inconclusive. We aimed to study the risk of hospitalization and death for COVID-19 in a large cohort of PWE from March 1, 2020 to October 31, 2021.
Methods: The historical cohort design (EpiLink Bologna) compared adult PWE grouped into people with focal epilepsy (PFE), idiopathic generalized epilepsy (PIGE), and developmental and/or epileptic encephalopathy (PDEE), and a population cohort matched (ratio 1:10) for age, sex, residence, and comorbidity (assessed with the multisource comorbidity score), living in the local health trust of Bologna (approximately 800 000 residents). Clinical data were linked to health administrative data.
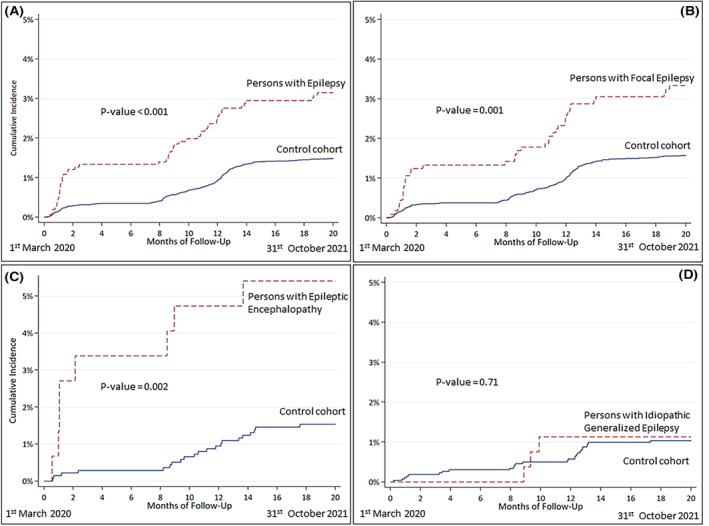
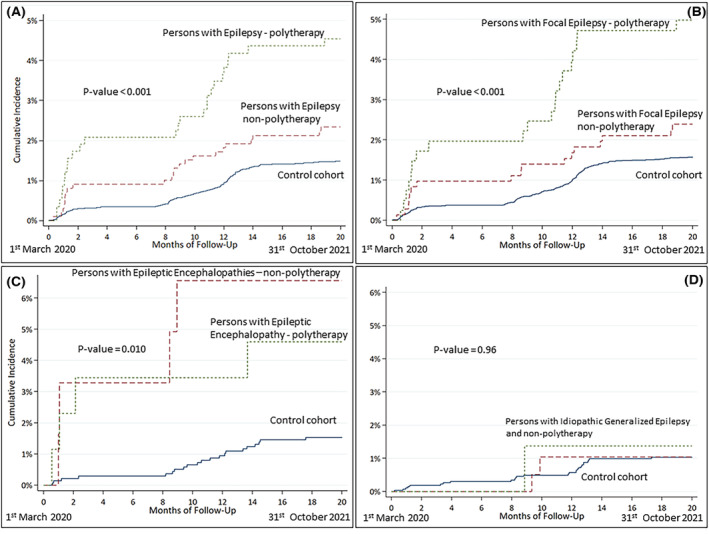
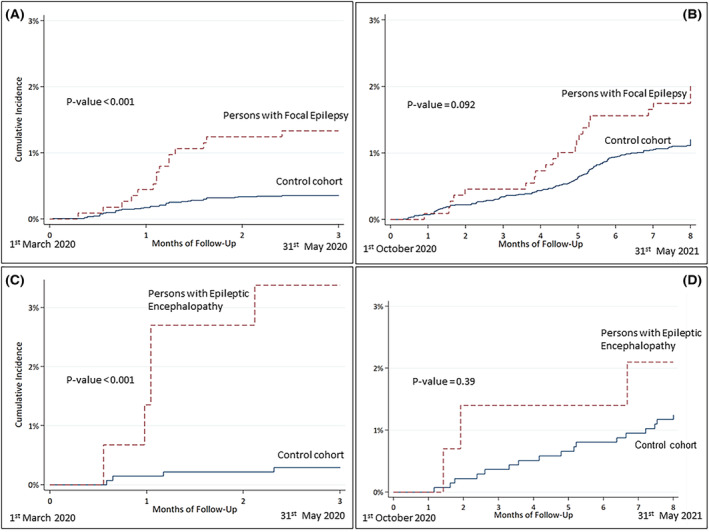
Results: In both cohorts (EpiLink: n = 1575 subjects, 1128 PFE, 267 PIGE, 148 PDEE, 32 other; controls: n = 15 326 subjects), 52% were females, and the mean age was 50 years (SD = 18). Hospital admissions for COVID-19 in the whole period were 49 (3.1%) in PWE and 225 (1.5%) in controls. The adjusted hazard ratio (aHR) in PWE was 1.9 (95% confidence interval [CI] = 1.4-2.7). The subgroups at higher risk were PFE (aHR = 1.9, 95% CI = 1.3-2.8) and PDEE (aHR = 3.9, 95% CI = 1.7-8.7), whereas PIGE had a risk comparable to the controls (aHR = 1.1, 95% CI = .3-3.5). Stratified analyses of the two main epidemic waves (March-May 2020, October 2020-May 2021) disclosed a higher risk of COVID-19-related hospitalization during the first epidemic wave (March-May 2020; aHR = 3.8, 95% CI = 2.2-6.7). Polytherapy with antiseizure medications contributed to a higher risk of hospital admission. Thirty-day risk of death after hospitalization was 14% in both PWE and controls.
Significance: During the first 20 months since the outbreak of COVID-19 in Bologna, PWE had a doubled risk of COVID-19 hospital admission compared to a matched control population. Conversely, epilepsy did not represent a risk factor for COVID-19-related death.
Keywords: antiseizure medication (ASM); epidemiology; epileptic encephalopathy; mortality; outcome.
© 2022 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflict of interest to disclose. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures