

Surgical treatment of rectovaginal fistula-predictors of outcome and effects on quality of life
- PMID: 35779081
- PMCID: PMC9262790
- DOI: 10.1007/s00384-022-04206-7
Surgical treatment of rectovaginal fistula-predictors of outcome and effects on quality of life
Abstract
Purpose: To determine the results after rectovaginal fistula (RVF) repair and find predictors of outcome. Primary objective was fistula healing. Secondary outcomes were morbidity and patient health-related quality of life (HRQoL).
Method: An observational study of 55 women who underwent RVF repair including both local procedures and tissue transposition 2003-2018 was performed. Baseline patient and fistula characteristics were registered, combined with a prospective HRQoL follow-up and a general questionnaire describing fistula symptoms.
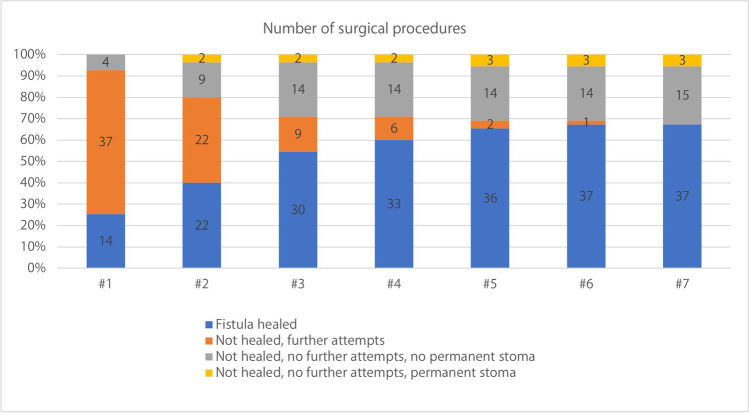
Results: Healing rate after index surgery was 25.5% (n = 14) but the final healing rate was 67.3% (n = 37). Comparing the etiologies, traumatic fistulas (iatrogenic and obstetric) had the highest healing rates after index surgery (n = 11, 45.9%) and after repeated operations at final follow-up (n = 22, 91.7%) compared with fistulas of inflammatory fistulas (Crohn's disease, cryptoglandular infection, and anastomotic leakage) that had inferior healing rates after both index surgery (n = 7, 7.1%) and at final follow-up (n = 13, 46.4%). Fistulas of the category others (radiation damage and unknown etiology) included a small amount of patients with intermediate results at both index surgery (n = 1, 33.3%) and healing rate at last follow-up (n = 2, 66.7%). The differences were statistically significant for both index surgery (p = 0.004) and at final follow-up (p = 0.001). Unhealed patients scored lower than both healed patients and the normal population in 6/8 Rand-36 domains, but the differences were not statistically significant.
Conclusions: Most traumatic rectovaginal fistulas closed after repeated surgery whereas inflammatory fistulas had a poor prognosis. Low healing rates after local repairs suggest that tissue transfer might be indicated more early in the treatment process. Unhealed fistulas were associated with reduced quality of life. Trial registration Clinicaltrials.gov No. NCT05006586.
Keywords: Colorectal diseases; Colorectal surgery; Quality of life; Rectovaginal fistula; Vaginal diseases.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
