

The Association Between the Occurrence of Common Treatment-Emergent Adverse Events and Efficacy Outcomes After Lasmiditan Treatment of a Single Migraine Attack: Secondary Analyses from Four Pooled Randomized Clinical Trials
- PMID: 35779194
- PMCID: PMC9259541
- DOI: 10.1007/s40263-022-00928-y
The Association Between the Occurrence of Common Treatment-Emergent Adverse Events and Efficacy Outcomes After Lasmiditan Treatment of a Single Migraine Attack: Secondary Analyses from Four Pooled Randomized Clinical Trials
Abstract
Background: In controlled clinical trials, compared with placebo, a significantly greater proportion of participants using lasmiditan to treat a migraine attack achieved 2-h pain freedom (PF) and experienced ≥ 1 treatment-emergent adverse event (TEAE).
Objective: To better inform clinicians about treatment expectations by evaluating the association between TEAEs and efficacy outcomes after lasmiditan treatment.
Methods: Pooled data from SAMURAI, SPARTAN, MONONOFU, and CENTURION were analyzed. A common TEAE (CTEAE) was defined as occurring in ≥ 2% in the overall population. Central nervous system (CNS)-CTEAEs were based on Medical Dictionary for Regulatory Activities.
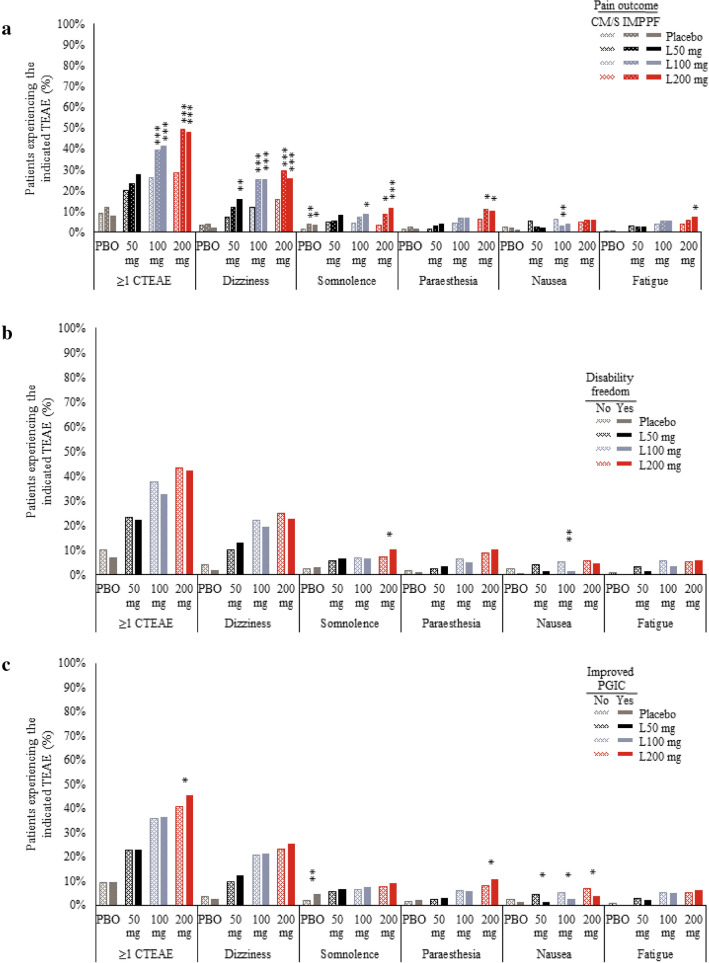
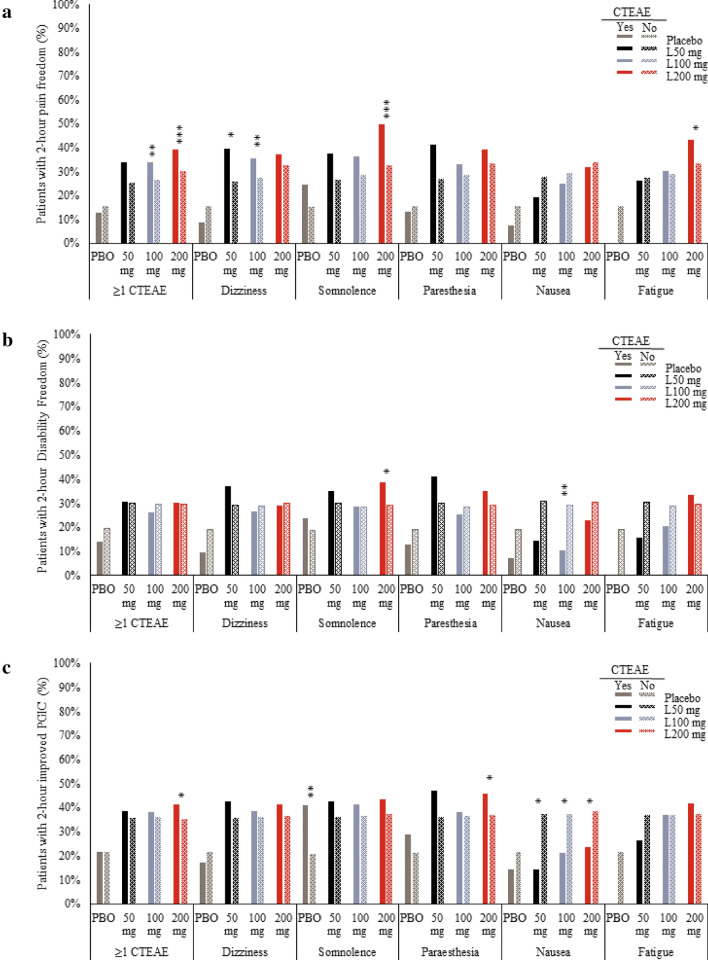
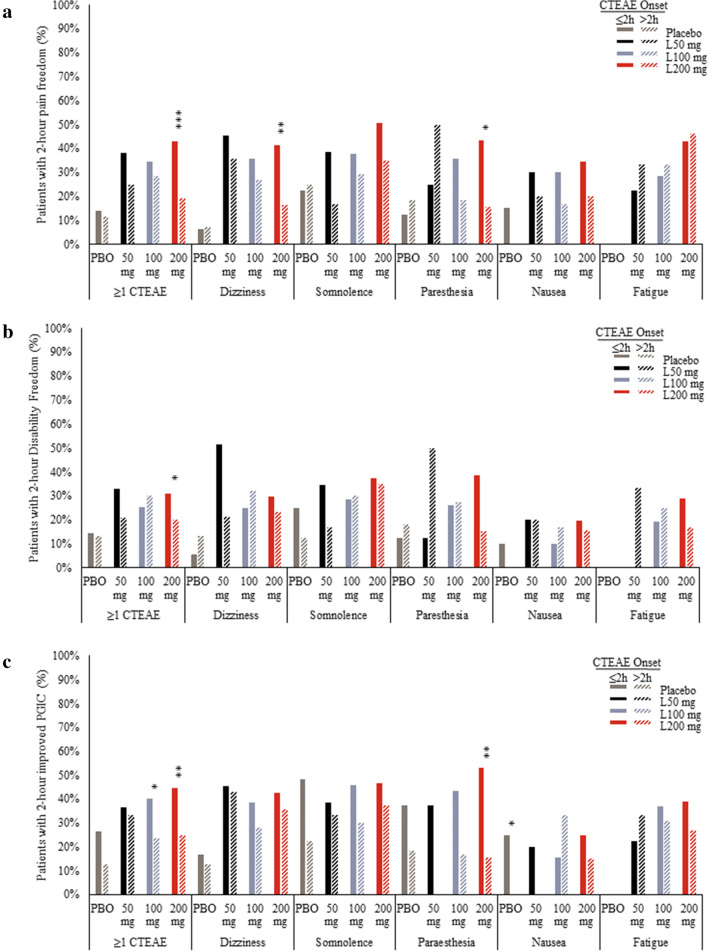
Results: At 2 h, a significantly higher percentage of lasmiditan 200 mg-treated participants who achieved PF experienced ≥ 1 CTEAE than non-responders who continued to experience moderate/severe pain (48.2% vs. 28.7%, respectively). Correspondingly, a significantly higher percentage of lasmiditan 200 mg-treated participants who experienced ≥ 1 CTEAE achieved PF at 2 h than those who did not (39.0% vs. 30.2%, respectively). Similar results were generally observed with individual CNS-CTEAEs, but for non-CNS-CTEAEs, this pattern was less evident or in the opposite direction. No consistent differences were observed for migraine-related functional disability freedom. The percentage of participants with improved patient global impression of change (PGIC) was greater with a CNS-CTEAE versus no CNS-CTEAE.
Conclusions: Those who had PF at 2 h were more likely to experience a CNS-CTEAE, and those with CNS-CTEAEs were more likely to experience PF. The occurrence of CTEAEs did not seem to negatively affect disability freedom or PGIC.
Gov registration: SAMURAI (NCT02439320), SPARTAN (NCT02605174), MONONOFU (NCT03962738), CENTURION (NCT03670810), ClinicalTrials.gov: NCT02439320, NCT02605174, NCT03962738, NCT03670810.
© 2022. Eli Lilly and Company.
Conflict of interest statement
RBL receives research support from the NIH, FDA, as well as the National Headache Foundation and the Marx Foundation. He also receives research support from Allergan/Abbvie, Amgen, Eli Lilly, and Electrocore. He receives personal fees as a consultant or advisor from Allergan/Abbvie, Amgen, Biohaven Holdings, Dr. Reddy's, GlaxoSmithKline, Grifols, Impel NeuroPharma, Eli Lilly, Lundbeck, Merck, Novartis, and Teva Pharmaceuticals. He holds stock or options in Biohaven Holdings, CtrlM Health and Manistee. EGD, PMH, JHK, MK, AMH, and YD are employees and minor stockholders of Eli Lilly and Company.
Figures

References
-
- Ashina M, Vasudeva R, Jin L, et al. Onset of efficacy following oral treatment with lasmiditan for the acute treatment of migraine: integrated results from 2 randomized double-blind placebo-controlled phase 3 clinical studies. Headache. 2019;59(10):1788–1801. doi: 10.1111/head.13636. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
