

Improving Treatment Options for Primary Hyperoxaluria
- PMID: 35779234
- PMCID: PMC9329168
- DOI: 10.1007/s40265-022-01735-x
Improving Treatment Options for Primary Hyperoxaluria
Abstract
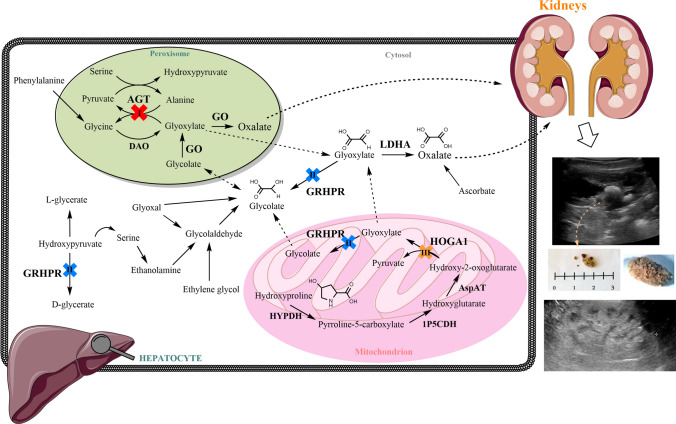
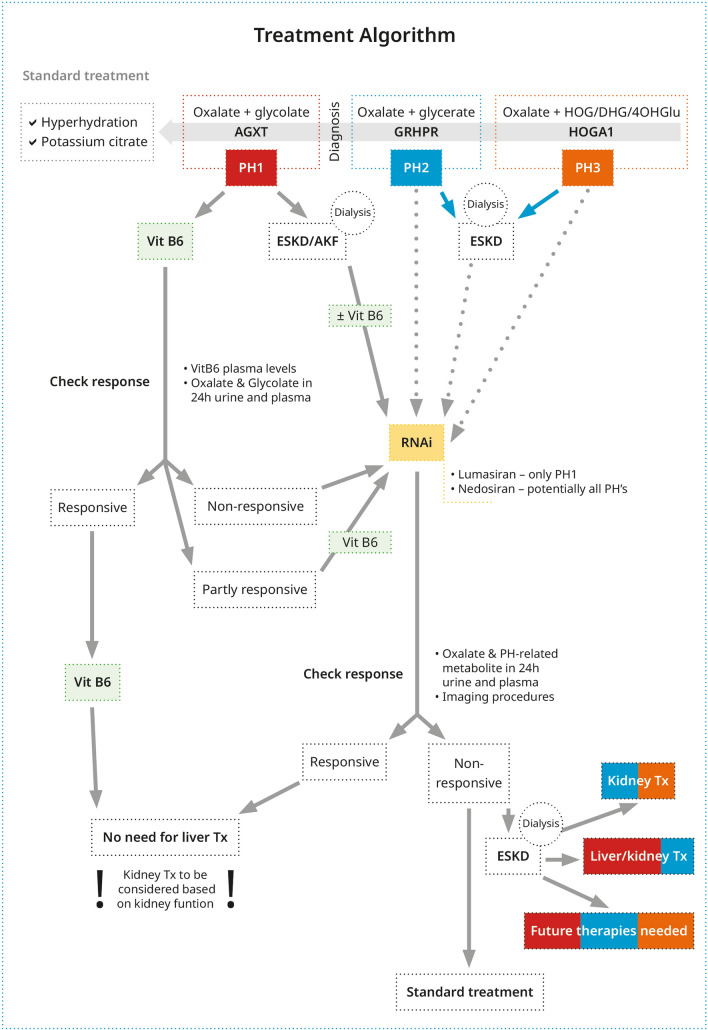
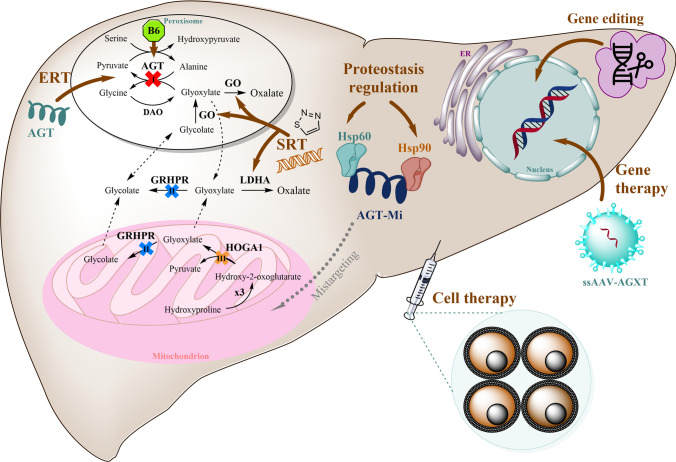
The primary hyperoxalurias are three rare inborn errors of the glyoxylate metabolism in the liver, which lead to massively increased endogenous oxalate production, thus elevating urinary oxalate excretion and, based on that, recurrent urolithiasis and/or progressive nephrocalcinosis. Frequently, especially in type 1 primary hyperoxaluria, early end-stage renal failure occurs. Treatment possibilities are scare, namely, hyperhydration and alkaline citrate medication. In type 1 primary hyperoxaluria, vitamin B6, though, is helpful in patients with specific missense or mistargeting mutations. In those vitamin B6 responsive, urinary oxalate excretion and concomitantly urinary glycolate is significantly decreased, or even normalized. In patients non-responsive to vitamin B6, RNA interference medication is now available. Lumasiran® is already available on prescription and targets the messenger RNA of glycolate oxidase, thus blocking the conversion of glycolate into glyoxylate, hence decreasing oxalate, but increasing glycolate production. Nedosiran blocks liver-specific lactate dehydrogenase A and thus the final step of oxalate production. Similar to vitamin B6 treatment, where both RNA interference urinary oxalate excretion can be (near) normalized and plasma oxalate decreases, however, urinary and plasma glycolate increases with lumasiran treatment. Future treatment possibilities are on the horizon, for example, substrate reduction therapy with small molecules or gene editing, induced pluripotent stem cell-derived autologous hepatocyte-like cell transplantation, or gene therapy with newly developed vector technologies. This review provides an overview of current and especially new and future treatment options.
© 2022. The Author(s).
Conflict of interest statement
Bernd Hoppe is an employee of Dicerna/Novo Nordisk. Cristina Martin-Higueras is a consultant of Dicerna/Novo Nordisk. There are no additional conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
