

Outsourcing health-care services to the private sector and treatable mortality rates in England, 2013-20: an observational study of NHS privatisation
- PMID: 35779546
- PMCID: PMC10932752
- DOI: 10.1016/S2468-2667(22)00133-5
Outsourcing health-care services to the private sector and treatable mortality rates in England, 2013-20: an observational study of NHS privatisation
Abstract
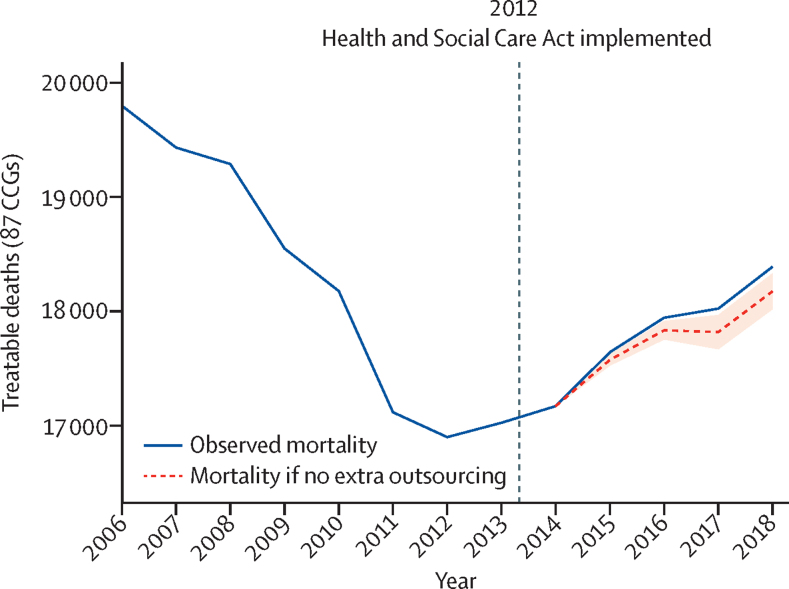
Background: The effects of outsourcing health services to for-profit providers are contested, with some arguing that introducing such providers will improve performance through additional competition while others worry that this will lead to cost cutting and poorer outcomes for patients. We aimed to examine this debate by empirically evaluating the impact of outsourced spending to private providers, following the 2012 Health and Social Care Act, on treatable mortality rates and the quality of health-care services in England.
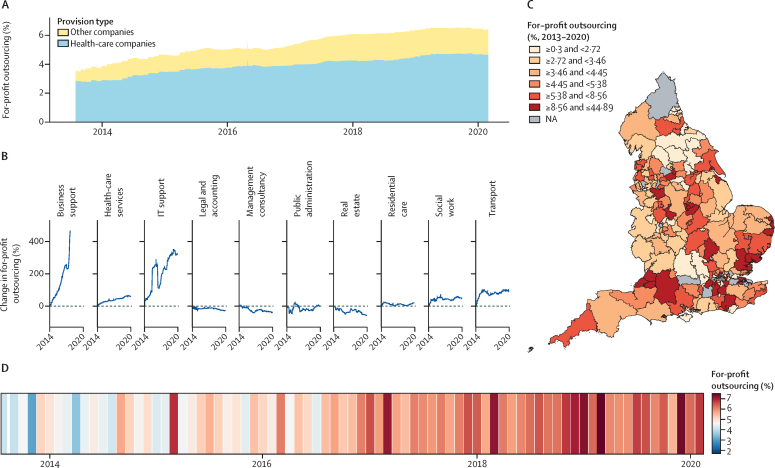
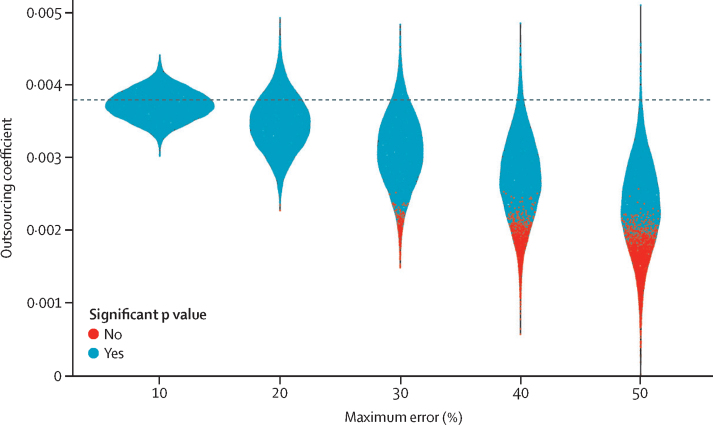
Methods: For this observational study, we used a novel database composed of parsable procurement contracts between April 1, 2013, and Feb 29, 2020 (n=645 674, value >£25 000, total value £204·1 billion), across 173 clinical commissioning groups (CCGs; regional health boards) in England. Data were compiled from 12 709 heterogenous expenditure files primarily scraped from commissioner websites with supplier names matched to registers identifying them as National Health Service (NHS) organisations, for-profit companies, or charities. We supplemented these data with rates of local mortality from causes that should be treatable by medical intervention, indicating the quality of health-care services. We used multivariate longitudinal regression models with fixed effects at the CCG level to analyse the association of for-profit outsourcing on treatable mortality rates in the following year. We used the average marginal effects to estimate total additional deaths attributable to changes in for-profit outsourcing. We provided alternative model specifications to test the robustness of our findings, match on background characteristics, examine the potential impact of measurement error, and adjust for possible confounding factors such as population demographics, total CCG expenditure, and local authority expenditure.
Findings: We found that an annual increase of one percentage point of outsourcing to the private for-profit sector corresponded with an annual increase in treatable mortality of 0·38% (95% CI 0·22-0·55; p=0·0016) or 0·29 (95% CI 0·09-0·49; p=0·0041) deaths per 100 000 population in the following year. This finding was robust to matching on background characteristics, adjusting for possible confounding factors, and measurement error in our dataset. Changes to for-profit outsourcing since 2014 were associated with an additional 557 (95% CI 153-961) treatable deaths across the 173 CCGs.
Interpretation: The privatisation of the NHS in England, through the outsourcing of services to for-profit companies, consistently increased in 2013-20. Private sector outsourcing corresponded with significantly increased rates of treatable mortality, potentially as a result of a decline in the quality of health-care services.
Funding: Wellcome Trust.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
For-profit health care might be damaging population health.Lancet Public Health. 2022 Jul;7(7):e576-e577. doi: 10.1016/S2468-2667(22)00142-6. Lancet Public Health. 2022. PMID: 35779537 No abstract available.
References
-
- Goodwin N, Pinch S. Explaining geographical variations in the contracting out of NHS hospital ancillary services: a contextual approach. Environ Plann A. 1995;27:1397–1418.
-
- Elkomy S, Cookson G, Jones S. Cheap and dirty: the effect of contracting out cleaning on efficiency and effectiveness. Public Adm Rev. 2019;79:193–202.
-
- Gingrich JR. Cambridge University Press; Cambridge: 2011. Making markets in the welfare state: the politics of varying market reforms.
-
- Krachler N, Greer I. When does marketisation lead to privatisation? Profit-making in English health services after the 2012 Health and Social Care Act. Soc Sci Med. 2015;124:215–223. - PubMed
-
- Sanderson M, Allen P, Osipovic D. The regulation of competition in the National Health Service (NHS): what difference has the Health and Social Care Act 2012 made? Health Econ Policy Law. 2017;12:1–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
