

Thromboprophylactic low-molecular-weight heparin versus standard of care in unvaccinated, at-risk outpatients with COVID-19 (ETHIC): an open-label, multicentre, randomised, controlled, phase 3b trial
- PMID: 35779560
- PMCID: PMC9243570
- DOI: 10.1016/S2352-3026(22)00173-9
Thromboprophylactic low-molecular-weight heparin versus standard of care in unvaccinated, at-risk outpatients with COVID-19 (ETHIC): an open-label, multicentre, randomised, controlled, phase 3b trial
Abstract
Background: COVID-19 is associated with inflammation and an increased risk of thromboembolic complications. Prophylactic doses of low-molecular-weight heparin have been used in hospitalised and non-critically ill patients with COVID-19. We aimed to evaluate the efficacy and safety of prophylactic low-molecular-weight heparin (enoxaparin) versus standard of care (no enoxaparin) in at-risk outpatients with COVID-19.
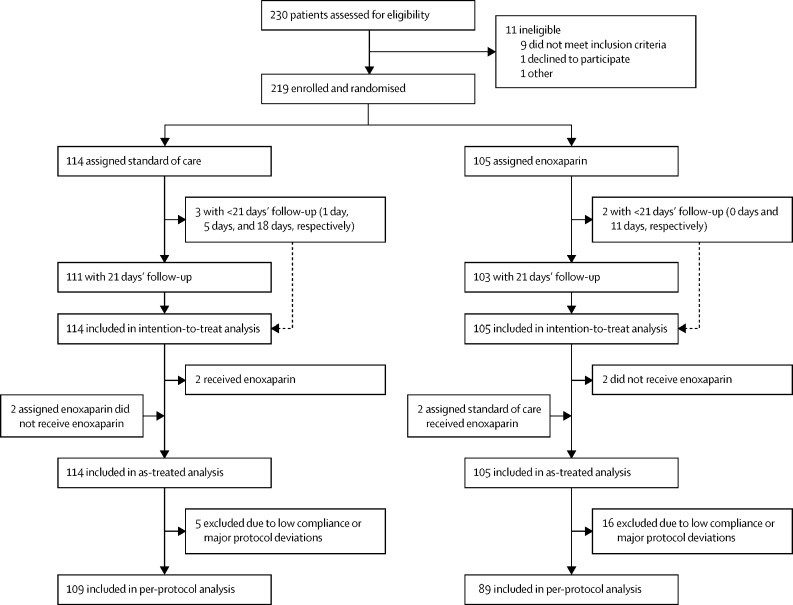
Methods: This open-label, multicentre, randomised, controlled, phase 3b trial (ETHIC) was done at 15 centres in six countries (Belgium, Brazil, India, South Africa, Spain, and the UK). We consecutively enrolled participants aged at least 30 years who had not received a COVID-19 vaccine and had symptomatic, confirmed COVID-19 in the outpatient setting plus at least one risk factor for severe disease. Within 9 days of symptom onset and by use of a web-based random block design (block size either 2 or 4), eligible participants were randomly assigned (1:1) to receive either subcutaneous enoxaparin for 21 days (40 mg once daily if they weighed <100 kg and 40 mg twice daily if they weighed ≥100 kg) or standard of care (without enoxaparin). The primary efficacy endpoint was the composite of all-cause hospitalisation and all-cause mortality at 21 days after randomisation and, in our main analysis, was analysed in the intention-to-treat population, which comprised all patients who were randomly assigned. Safety was also analysed in the intention-to-treat population for our main analysis. This trial is registered with ClinicalTrials.gov, NCT04492254, and is complete.
Findings: Following the advice of the Data and Safety Monitoring Board, this study was terminated early due to slow enrolment and a lower-than-expected event rate. Between Oct 27, 2020, and Nov 8, 2021, 230 patients with COVID-19 were assessed for eligibility, of whom 219 were enrolled and randomly assigned to receive standard of care (n=114) or enoxaparin (n=105). 96 (44%) patients were women, 122 (56%) were men, and one patient had missing sex data. 141 (65%) of 218 participants with data on race and ethnicity were White, 60 (28%) were Asian, and 16 (7%) were Black, mixed race, or Arab or Middle Eastern. Median follow-up in both groups was 21 days (IQR 21-21). There was no difference in the composite of all-cause mortality and hospitalisation at 21 days between the enoxaparin group (12 [11%] of 105 patients) and the standard-of-care group (12 [11%] of 114 patients; unadjusted hazard ratio 1·09 [95% CI 0·49-2·43]; log-rank p=0·83). At 21 days, two (2%) of 105 patients in the enoxaparin group (one minor bleed and one bleed of unknown severity) and one (1%) of 114 patients in the standard-of-care group (major abnormal uterine bleeding) had a bleeding event. 22 (21%) patients in the enoxaparin group and 13 (11%) patients in the standard-of-care group had adverse events. The most common adverse event in both groups was COVID-19-related pneumonia (six [6%] patients in the enoxaparin group and five [4%] patients in the standard-of-care group). One patient in the enoxaparin group died and their cause of death was unknown.
Interpretation: The ETHIC trial results suggest that prophylaxis with low-molecular-weight heparin had no benefit for at-risk outpatients with COVID-19. Although the trial was terminated early, our data, combined with data from similar studies, provide further insights to inform international guidelines and influence clinical practice.
Funding: The Thrombosis Research Institute and Sanofi UK.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests FC reports speaker fees from Boehringer Ingelheim Pharma, Bayer, Pfizer, and Daiichi-Sankyo Europe, and a modest research grant from Daiichi-Sankyo Europe. JS reports personal fees from Pfizer, AstraZeneca, Novartis, Sanofi, BMS, Dr Reddy's Laboratory, Lupin, and Abbot. RDL reports research grants from Bristol Myers Squibb, Pfizer, Amgen, GlaxoSmithKline, Medtronic, and Sanofi Aventis, and personal fees from Bristol Myers Squibb, Pfizer, Boehringer Ingelheim, and Bayer, outside the submitted work. BJ reports personal fees from Bayer HealthCare and Sanofi-Aventis. JIA reports speaker fees from Sanofi, Rovi, Bayer, and Aspen. FDRH acknowledges part support as Director of the National Institute for Health and Care Research (NIHR) Applied Research Collaboration Oxford Thames Valley and Theme Lead of the NIHR Oxford University Hospital Biomedical Research Centre, and has also received occasional fees or expenses for speaking or consultancy from AstraZeneca, Boehringer Ingelheim, Bayer, BMS/Pfizer, and Novartis. HG reports personal fees from Pfizer, Bayer, and Boehringer Ingelheim. PM reports honoraria from Bayer Pharma and Portolo. SS reports speaker fees from Bayer Pharma, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Sanofi Aventis, and Pfizer, and consultancy fees from Bayer Pharma, Boehringer Ingelheim, Daiichi Sankyo, Sanofi Aventis, Aspen, and Pfizer. SH reports personal fees from Bayer, Bristol Myers Squibb, Daiichi Sankyo, Portola, and Sanofi, outside the submitted work. AGGT reports grants from Bayer Healthcare and personal fees from Bayer Healthcare, Bristol Myers Squibb/Pfizer, Daiichi Sankyo, and Boehringer Ingelheim, outside the submitted work. WA reports honoraria from Bayer Pharma, Bristol Myers Squibb, Pfizer, Daiichi Sankyo, Portola, Aspen, Sanofi, Leo Pharma, Norgine, and Werfen. ATR reports consultancy fees from Bayer Pharma, Daiichi Sankyo, Sanofi, Aspen, and Pfizer. KP reports a consultancy fee from Johnson & Johnson. AKK reports research grants from Anthos, Bayer, and Sanofi and personal fees from Anthos Therapeutics, Bayer, and Sanofi. All other authors declare no competing interests.
Figures

References
-
- Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004;110(suppl 1):IV4–I12. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
