

Pilot of rapid implementation of the advanced practice provider in the workflow of an existing tele-critical care program
- PMID: 35780144
- PMCID: PMC9250728
- DOI: 10.1186/s12913-022-08251-4
Pilot of rapid implementation of the advanced practice provider in the workflow of an existing tele-critical care program
Abstract
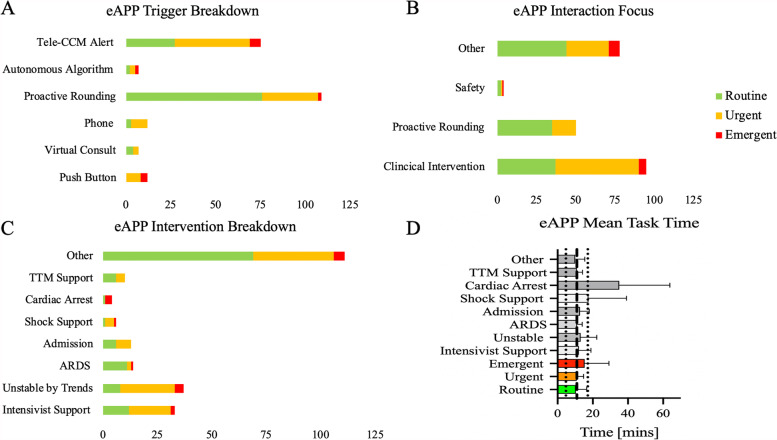
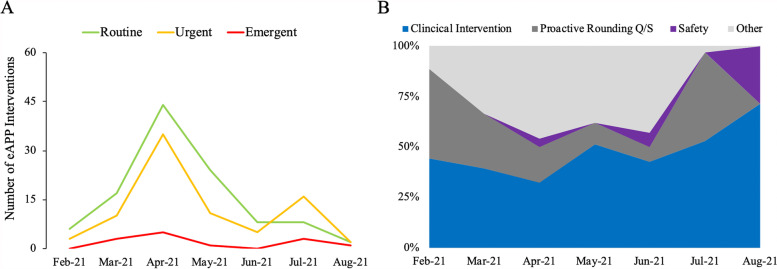
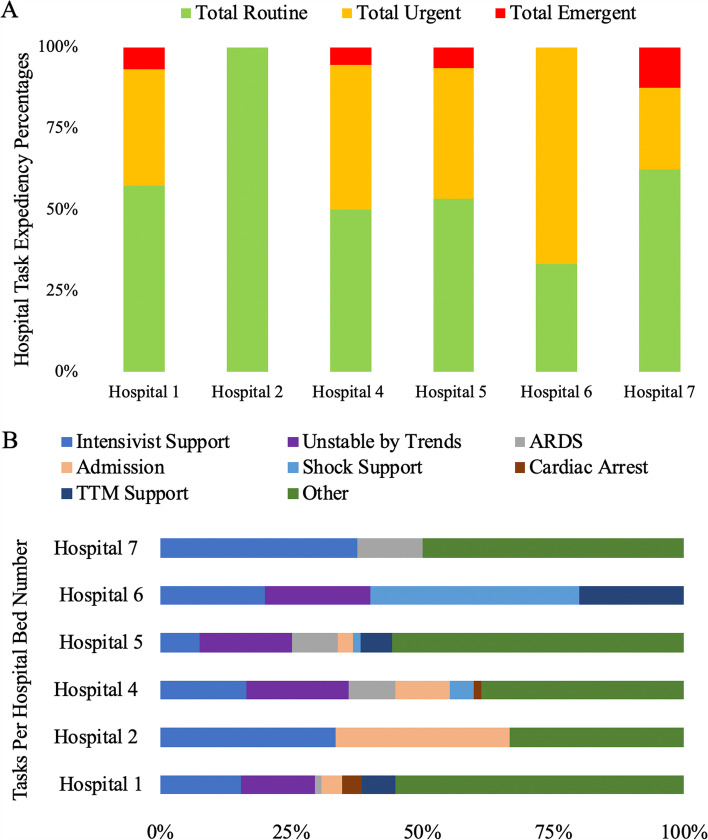
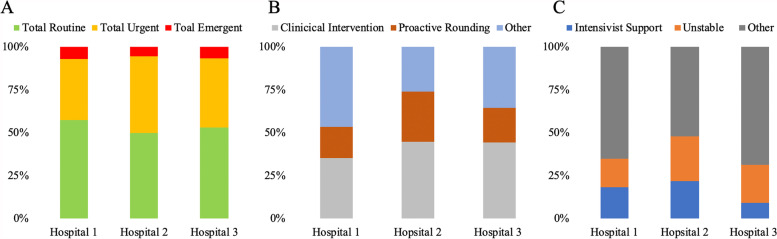
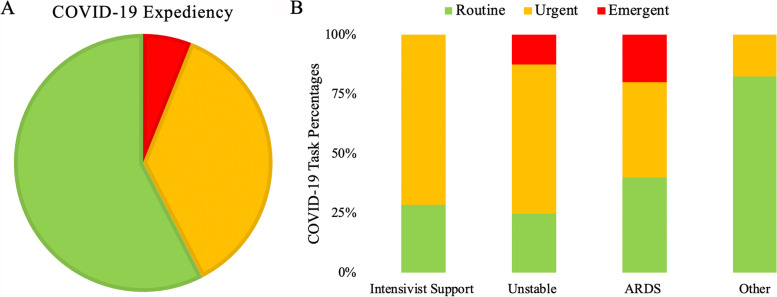
Incorporating the advanced practice provider (APP) in the delivery of tele critical care medicine (teleCCM) addresses the critical care provider shortage. However, the current literature lacks details of potential workflows, deployment difficulties and implementation outcomes while suggesting that expanding teleCCM service may be difficult. Here, we demonstrate the implementation of a telemedicine APP (eAPP) pilot service within an existing teleCCM program with the objective of determining the feasibility and ease of deployment. The goal is to augment an existing tele-ICU system with a balanced APP service to assess the feasibility and potential impact on the ICU performance in several hospitals affiliated within a large academic center. A REDCap survey was used to assess eAPP workflows, expediency of interventions, duration of tasks, and types of assignments within different service locations. Between 02/01/2021 and 08/31/2021, 204 interventions (across 133 12-h shift) were recorded by eAPP (nroutine = 109 (53.4%); nurgent = 82 (40.2%); nemergent = 13 (6.4%). The average task duration was 10.9 ± 6.22 min, but there was a significant difference based on the expediency of the task (F [2; 202] = 3.89; p < 0.022) and type of tasks (F [7; 220] = 6.69; p < 0.001). Furthermore, the eAPP task type and expediency varied depending upon the unit engaged and timeframe since implementation. The eAPP interventions were effectively communicated with bedside staff with only 0.5% of suggestions rejected. Only in 2% cases did the eAPP report distress. In summary, the eAPP can be rapidly deployed in existing teleCCM settings, providing adaptable and valuable care that addresses the specific needs of different ICUs while simultaneously enhancing the delivery of ICU care. Further studies are needed to quantify the input more robustly.
Keywords: Advance practice providers; ICU; Implementation; Operations; Tele-critical care medicine; Workflow.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
