

Ventilatory settings in the initial 72 h and their association with outcome in out-of-hospital cardiac arrest patients: a preplanned secondary analysis of the targeted hypothermia versus targeted normothermia after out-of-hospital cardiac arrest (TTM2) trial
- PMID: 35780195
- PMCID: PMC9304050
- DOI: 10.1007/s00134-022-06756-4
Ventilatory settings in the initial 72 h and their association with outcome in out-of-hospital cardiac arrest patients: a preplanned secondary analysis of the targeted hypothermia versus targeted normothermia after out-of-hospital cardiac arrest (TTM2) trial
Abstract
Purpose: The optimal ventilatory settings in patients after cardiac arrest and their association with outcome remain unclear. The aim of this study was to describe the ventilatory settings applied in the first 72 h of mechanical ventilation in patients after out-of-hospital cardiac arrest and their association with 6-month outcomes.
Methods: Preplanned sub-analysis of the Target Temperature Management-2 trial. Clinical outcomes were mortality and functional status (assessed by the Modified Rankin Scale) 6 months after randomization.
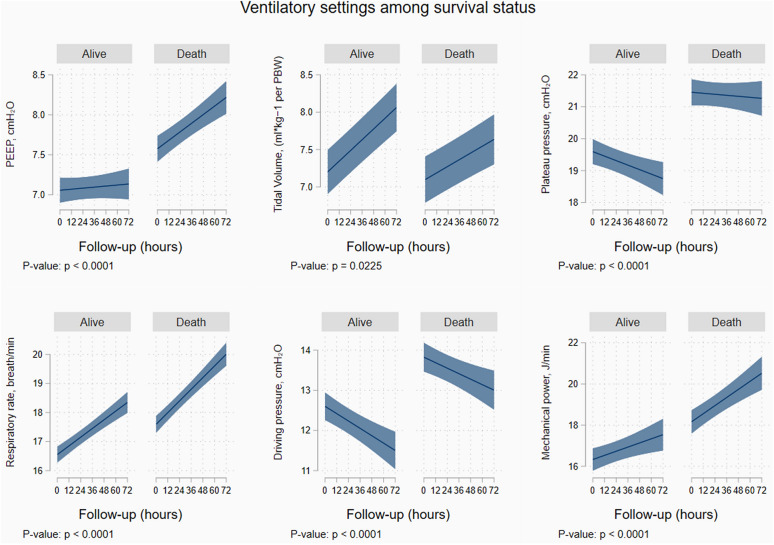
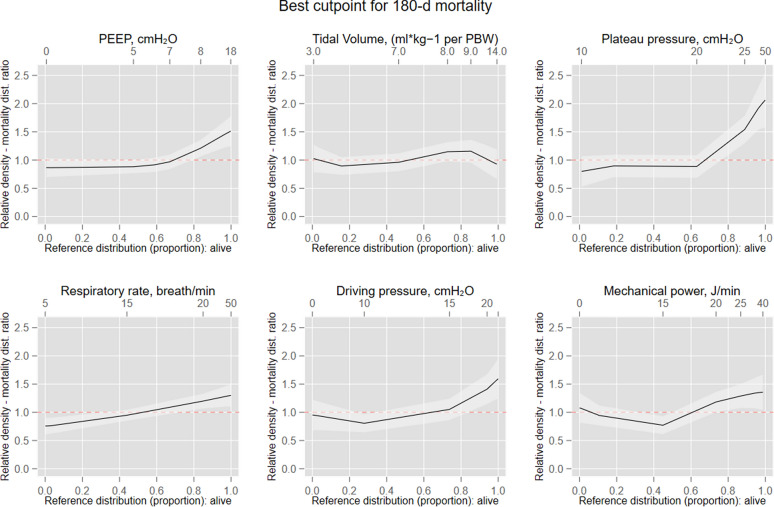
Results: A total of 1848 patients were included (mean age 64 [Standard Deviation, SD = 14] years). At 6 months, 950 (51%) patients were alive and 898 (49%) were dead. Median tidal volume (VT) was 7 (Interquartile range, IQR = 6.2-8.5) mL per Predicted Body Weight (PBW), positive end expiratory pressure (PEEP) was 7 (IQR = 5-9) cmH20, plateau pressure was 20 cmH20 (IQR = 17-23), driving pressure was 12 cmH20 (IQR = 10-15), mechanical power 16.2 J/min (IQR = 12.1-21.8), ventilatory ratio was 1.27 (IQR = 1.04-1.6), and respiratory rate was 17 breaths/minute (IQR = 14-20). Median partial pressure of oxygen was 87 mmHg (IQR = 75-105), and partial pressure of carbon dioxide was 40.5 mmHg (IQR = 36-45.7). Respiratory rate, driving pressure, and mechanical power were independently associated with 6-month mortality (omnibus p-values for their non-linear trajectories: p < 0.0001, p = 0.026, and p = 0.029, respectively). Respiratory rate and driving pressure were also independently associated with poor neurological outcome (odds ratio, OR = 1.035, 95% confidence interval, CI = 1.003-1.068, p = 0.030, and OR = 1.005, 95% CI = 1.001-1.036, p = 0.048). A composite formula calculated as [(4*driving pressure) + respiratory rate] was independently associated with mortality and poor neurological outcome.
Conclusions: Protective ventilation strategies are commonly applied in patients after cardiac arrest. Ventilator settings in the first 72 h after hospital admission, in particular driving pressure and respiratory rate, may influence 6-month outcomes.
Trial registration: ClinicalTrials.gov NCT02908308.
Keywords: Cardiac arrest; Driving pressure; Mechanical power; Mechanical ventilation; Outcome; Ventilator settings.
© 2022. The Author(s).
Conflict of interest statement
MS, receiving consulting fees from Bard Medical; PJY, receiving lecture fees from Bard Medical; FST, receiving grant support from Bard Medical and ZOLL Medical; AN, receiving grant support, paid to University College Dublin, from AM Pharma and grant sup-port, paid to Monash University, from Baxter Healthcare; MSC, receiving lecture fees from Edwards Lifesciences; HF, receiving fees for academic advising from TEQCool; and NN, receiving lecture fees from Bard Medical and consulting fees from BrainCool. RB is supported by INCLIVA. No other potential conflict of interest relevant to this article was reported.
Figures

Comment in
-
The importance of ventilator settings and respiratory mechanics in patients resuscitated from cardiac arrest.Intensive Care Med. 2022 Aug;48(8):1056-1058. doi: 10.1007/s00134-022-06779-x. Epub 2022 Jul 1. Intensive Care Med. 2022. PMID: 35776161 No abstract available.
-
Airway management in cardiac arrest and outcomes.Intensive Care Med. 2022 Dec;48(12):1827-1828. doi: 10.1007/s00134-022-06878-9. Epub 2022 Sep 29. Intensive Care Med. 2022. PMID: 36173413 No abstract available.
References
-
- Kim Y-M, Yim H-W, Jeong S-H, Klem ML, Callaway CW. Does therapeutic hypothermia benefit adult cardiac arrest patients presenting with non-shockable initial rhythms? A systematic review and meta-analysis of randomized and non-randomized studies. Resuscitation. 2012;83:188–196. - PubMed
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788. - PubMed
-
- Neto AS, Barbas CSV, Simonis FD, Artigas-Raventós A, Canet J, Determann RM, et al. Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): an international, multicentre, prospective study. Lancet Respir Med. 2016;4:882–893. - PubMed
