

Network analysis of comorbid depression and anxiety and their associations with quality of life among clinicians in public hospitals during the late stage of the COVID-19 pandemic in China
- PMID: 35780965
- PMCID: PMC9242942
- DOI: 10.1016/j.jad.2022.06.051
Network analysis of comorbid depression and anxiety and their associations with quality of life among clinicians in public hospitals during the late stage of the COVID-19 pandemic in China
Abstract
Background: Mental health problems are common among clinicians working in public hospitals even in the late stage of the COVID-19 pandemic. Network analysis is a novel approach to explore interactions between mental health problems at the symptom level. This study examined the network structure of comorbid depression and anxiety and their associations with quality of life (QOL) among hospital clinicians in China during the late stage of the COVID-19 pandemic.
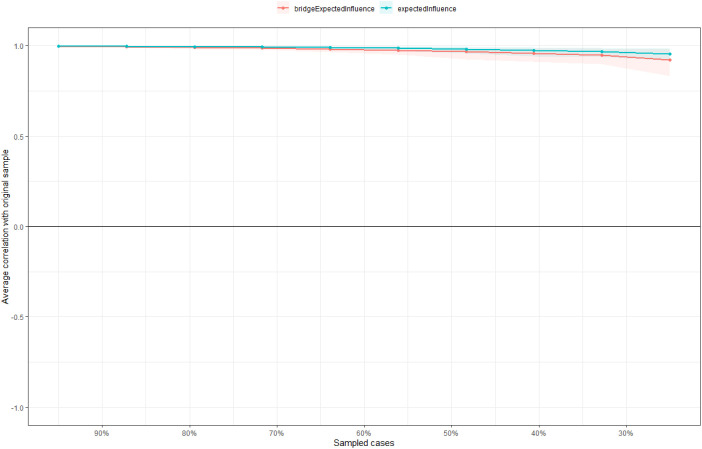
Methods: A total of 4931 participants were recruited from October 13 to 22, 2020. The nine-item Patient Health Questionnaire (PHQ-9), seven-item Generalized Anxiety Disorder Scale (GAD-7), and the World Health Organization Quality of Life Questionnaire-Brief Version (WHOQOL-BREF) were used to measure depressive and anxiety symptoms, and QOL, respectively. Central and bridge symptoms were identified with centrality and bridge centrality indices, respectively. Network stability was examined using the case-dropping procedure.
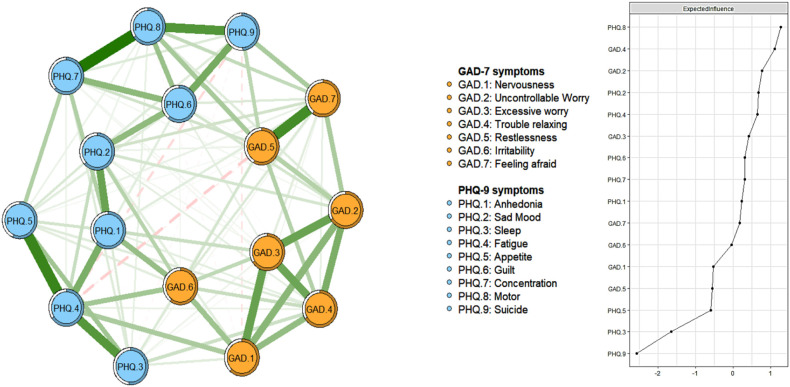
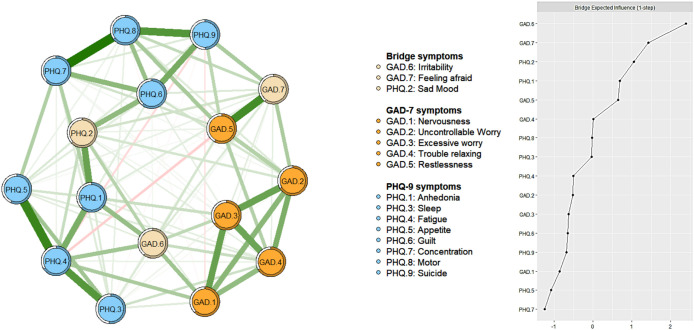
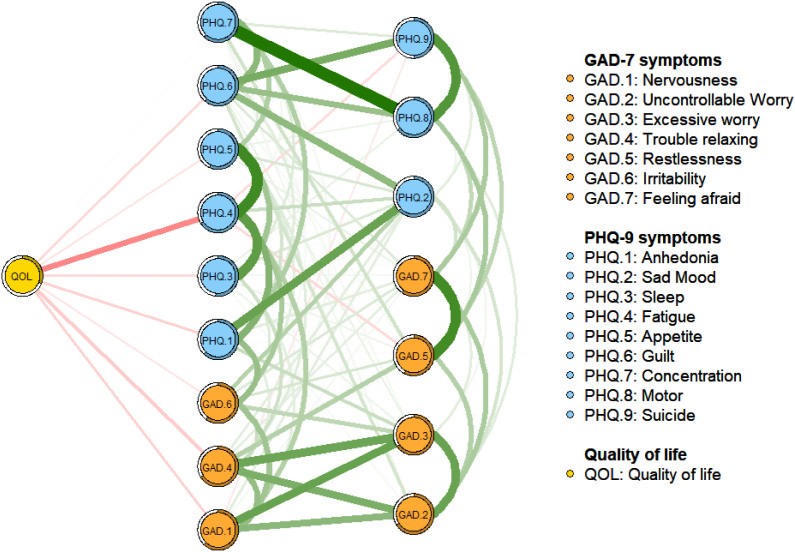
Results: The prevalence of depression (defined as PHQ-9 total score ≥ 5) was 35.1 % [95 % confidence interval (CI) = 33.73-36.41 %)], the prevalence of anxiety (GAD-7 total score ≥ 5) was 32.5 % (95 % CI = 31.20-33.84 %), while the prevalence of comorbid depression and anxiety was 26.9 % (95 % CI = 25.7-28.2 %). "Impaired motor skills", "Trouble relaxing" and "Uncontrollable worry" were the central symptoms in the whole depression-anxiety network. "Irritability", "Feeling afraid" and "Sad mood" were the most key bridge symptoms linking depression and anxiety. Three symptoms ("Fatigue", "Trouble relaxing" and "Nervousness") were the most strongly and negatively associated with QOL. Neither gender nor the experiences of caring for COVID-19 patients was associated with network global strength, distribution of edge weights or individual edge weights.
Limitations: The causality between variables could not be established. Depressive and anxiety symptoms were assessed by self-report measures, which may result in recall bias and limitations in capturing clinical phenomena.
Conclusions: Both the central (i.e., "Impaired motor skills", "Trouble relaxing" and "Uncontrollable worry") and bridge symptoms (i.e., "Irritability", "Feeling afraid" and "Sad mood") identified in this network analysis should be targeted in specific treatment and preventive measures for comorbid depressive and anxiety symptoms among clinicians in the late stage of the pandemic. Furthermore, "Fatigue", "Trouble relaxing" and "Nervousness" are key symptoms to address to improve clinicians' QOL.
Keywords: Anxiety; COVID-19; Clinicians; Depression; Network analysis.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
None.
Figures
Similar articles
-
Network analysis of anxiety and depressive symptoms among nursing students during the COVID-19 pandemic.J Affect Disord. 2021 Nov 1;294:753-760. doi: 10.1016/j.jad.2021.07.072. Epub 2021 Jul 22. J Affect Disord. 2021. PMID: 34375200 Free PMC article.
-
Anxiety and depressive symptoms in college students during the late stage of the COVID-19 outbreak: a network approach.Transl Psychiatry. 2021 Dec 17;11(1):638. doi: 10.1038/s41398-021-01738-4. Transl Psychiatry. 2021. PMID: 34921138 Free PMC article.
-
Depression and anxiety among caregivers of psychiatric patients during the late stage of the COVID-19 pandemic: A perspective from network analysis.J Affect Disord. 2024 Jan 1;344:33-40. doi: 10.1016/j.jad.2023.09.034. Epub 2023 Oct 2. J Affect Disord. 2024. PMID: 37793475
-
A network analysis of the interrelationships between depression, anxiety, insomnia and quality of life among fire service recruits.Front Public Health. 2024 Jul 3;12:1348870. doi: 10.3389/fpubh.2024.1348870. eCollection 2024. Front Public Health. 2024. PMID: 39022427 Free PMC article.
-
A network model of depressive and anxiety symptoms: a statistical evaluation.Mol Psychiatry. 2024 Mar;29(3):767-781. doi: 10.1038/s41380-023-02369-5. Epub 2024 Jan 18. Mol Psychiatry. 2024. PMID: 38238548 Free PMC article.
Cited by
-
Network analysis of depression and anxiety symptoms and their associations with cognitive fusion among pregnant women.BMC Psychiatry. 2025 May 26;25(1):537. doi: 10.1186/s12888-025-06978-y. BMC Psychiatry. 2025. PMID: 40420034 Free PMC article.
-
Mental health impact on patients with COVID-19 in the community under a long period of full lockdown in Vietnam.J Int Med Res. 2024 Jan;52(1):3000605231221087. doi: 10.1177/03000605231221087. J Int Med Res. 2024. PMID: 38259217 Free PMC article.
-
Network analysis of depressive and anxiety symptoms in older Chinese adults with diabetes mellitus.Front Psychiatry. 2024 Jan 29;15:1328857. doi: 10.3389/fpsyt.2024.1328857. eCollection 2024. Front Psychiatry. 2024. PMID: 38347882 Free PMC article.
-
Network analysis of depression and anxiety symptoms and their associations with mobile phone addiction among Chinese medical students during the late stage of the COVID-19 pandemic.SSM Popul Health. 2023 Nov 23;25:101567. doi: 10.1016/j.ssmph.2023.101567. eCollection 2024 Mar. SSM Popul Health. 2023. PMID: 38524176 Free PMC article.
-
Prevalence of COVID-19 fear and its association with quality of life and network structure among Chinese mental health professionals after ending China's dynamic zero-COVID policy: a national survey.Front Public Health. 2023 Oct 30;11:1280688. doi: 10.3389/fpubh.2023.1280688. eCollection 2023. Front Public Health. 2023. PMID: 37965522 Free PMC article.
References
-
- Aiken L.H., Clarke S.P., Sloane D.M., Sochalski J., Silber J.H. Hospital nurse staffing and patient mortality, nurse burnout, and job dissatisfaction. JAMA. 2002;288(16):1987–1993. - PubMed
-
- An Y., et al. Mirtazapine exerts an anxiolytic-like effect through activation of the median raphe nucleus-dorsal hippocampal 5-HT pathway in contextual fear conditioning in rats. Prog. Neuro-Psychopharmacol. Biol. Psychiatry. 2016;70:17–23. - PubMed
-
- Angermeyer M.C., Holzinger A., Matschinger H., Stengler-Wenzke K. Depression and quality of life: results of a follow-up study. Int J Soc Psychiatry. 2002;48(3):189–199. - PubMed
-
- Baker A.L., Thornton L.K., Hiles S., Hides L., Lubman D.I. Psychological interventions for alcohol misuse among people with co-occurring depression or anxiety disorders: a systematic review. J. Affect. Disord. 2012;139(3):217–229. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
