

De-Prescribing Proton Pump Inhibitors in Patients With End Stage Kidney Disease: A Quality Improvement Project
- PMID: 35782023
- PMCID: PMC9243371
- DOI: 10.1177/20543581221106244
De-Prescribing Proton Pump Inhibitors in Patients With End Stage Kidney Disease: A Quality Improvement Project
Abstract
Background: Proton pump inhibitors (PPIs) are widely prescribed and may be associated with harm; hypomagnesemia and reduced effectiveness of calcium carbonate phosphate binders may be important in end-stage kidney disease (ESKD).
Objectives: Our objectives included (1) discontinuing PPIs and H2 blockers and (2) assessing the impact on serum magnesium and markers of mineral metabolism.
Design: Prospective cohort.
Setting: Satellite hemodialysis unit of a tertiary care hospital.
Patients: Incident and prevalent patients with ESKD treated with hemodialysis.
Measurements: We assessed the impact of stopping PPI/H2 blockers in patients who did not have an absolute indication as per guidelines in the general population; serum magnesium, calcium, and phosphate were measured before and approximately 8 weeks later. Analysis of variance (ANOVA) test and Kruskal-Wallis was used to describe the population. Wilcoxon signed rank test for the paired change scores (from pre to post).
Methods: The electronic medical record (EMR) was extensively searched for absolute indications for a PPI. Results were reviewed with the primary nephrology team before approaching patients about stopping the PPI. Basic demographic information and select medications were also collected.
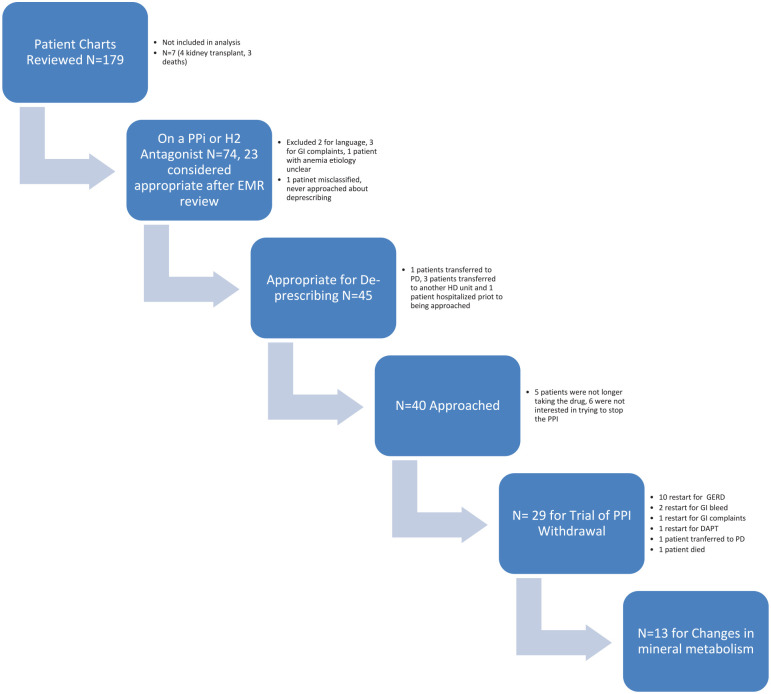
Results: Electronic medical records were reviewed for 179 patients, 74 had a PPI or H2 antagonist or both on their medication list (43%); 23 (31%) were assessed as appropriate. After primary team and patient review, 29 patients agreed to a trial of PPI withdrawal. Fourteen patients restarted their PPI, most for gastroesophageal reflux disease. Three patients had a GI bleed, 1 fatally. Serum calcium (P = .17) and the dose of phosphate binders (P = .075) did not change but serum phosphate increased (1.55 [0.29] to 1.85 [0.34] mmol/L; P = .0005). Serum magnesium also increased (1.01 [0.16] to 1.06 [0.14] mmol/L; P = .01).
Limitations: Small patient numbers and observational nature of the study does not establish causation in this population at high risk to experience a gastrointestinal bleed.
Conclusions: Our results suggest that PPI deprescribing as recommended in the general population may be associated with harm in patients with ESKD and requires further study.
Trial registration: Not registered.
Contexte: Les inhibiteurs de la pompe à protons (IPP) sont largement prescrits et peuvent être associés à une atteinte rénale; l’hypomagnésémie et la réduction de l’efficacité des chélateurs de phosphate à base de carbonate de calcium peuvent devenir significatifs chez les patients avec insuffisance rénale terminale (IRT).
Objectifs: Nos objectifs comprenaient 1) l’arrêt des IPP et des antagonistes H2 et 2) l’évaluation des conséquences sur le taux de magnésium sérique et les marqueurs du métabolisme minéral.
Conception: Étude de cohorte prospective.
Cadre: L’unité d’hémodialyse satellite d’un hôpital de soins tertiaires.
Sujets: Patients incidents et prévalents atteints d’IRT et traités par hémodialyse.
Mesures: Nous avons évalué les conséquences de l’arrêt des IPP et antagonistes H2 chez les patients qui n’avaient pas d’indication absolue pour ces médicaments, conformément aux directives pour la population générale. Les taux sériques de magnésium, de calcium et de phosphate ont été mesurés avant l’arrêt et environ huit semaines plus tard. Les tests ANOVA et Kruskal-Wallis ont été utilisés pour décrire la population, et le test de rang de Wilcoxon pour les scores de changement appariés (de pré à post-intervention).
Méthodologie: Les dossiers médicaux électroniques (DMÉ) ont été consultés rigoureusement à la recherche d’une indication absolue pour un IPP. Les résultats ont été revus avec l’équipe de néphrologie primaire avant d’approcher les patients quant à un arrêt des IPP. Les données démographiques initiales et les prescriptions pour certains médicaments ont également été recueillies.
Résultats: Les DMÉ de 179 patients ont été consultés, révélant que 74 (43 %) d’entre eux prenaient soit un IPP, soit un antagoniste H2, soit les deux; chez 23 patients (31 %) la prescription était appropriée. Après évaluation par l’équipe médicale et discussion avec les patients, 29 patients ont accepté de cesser l’IPP. Quatorze patients ont recommencé les IPP, la plupart pour un reflux gastro-œsophagien. Trois patients ont souffert d’une hémorragie gastro-intestinale, dont une s’est avérée fatale. Le taux de calcium sérique (p=0,17) et la dose de chélateurs du phosphate (p=0,075) n’ont pas changé, mais le taux de phosphate sérique a augmenté (1,55 [0,29] à 1,85 [0,34] mmol/L; p=0,0005), tout comme le taux de magnésium sérique (1,01 [0,16] à 1,06 [0,14] mmol/L; p=0,01).
Limites: Le faible échantillon de patients et la nature observationnelle de l’étude ne permettent pas d’établir un lien de causalité dans cette population présentant un risque élevé d’hémorragie gastro-intestinale.
Conclusion: Nos résultats suggèrent que la déprescription des IPP recommandée dans la population générale pourrait être associée à un préjudice chez les patients atteints d’IRT. Des études plus approfondies sont nécessaires.
Enregistrement de l’essai: Non enregistré.
Keywords: deprescribing; hemodialysis; mineral metabolism; proton pump inhibitors; quality improvement.
© The Author(s) 2022.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. D Zimmerman has received financial support from Otsuka as a speaker and advisory board member. She has also received financial support from Bayer as an advisory board member. The other authors do not have any disclosures to declare.
Figures
Similar articles
-
Appropriateness of Antiplatelet Therapy and Proton Pump Inhibitor Prescribing in End-Stage Kidney Disease: A Retrospective Quality Investigation Study.Can J Kidney Health Dis. 2025 Jan 6;12:20543581241312618. doi: 10.1177/20543581241312618. eCollection 2025. Can J Kidney Health Dis. 2025. PMID: 39764378 Free PMC article.
-
AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review.Gastroenterology. 2022 Apr;162(4):1334-1342. doi: 10.1053/j.gastro.2021.12.247. Epub 2022 Feb 17. Gastroenterology. 2022. PMID: 35183361 Review.
-
Proton pump inhibitors and hypomagnesemia in the general population: a population-based cohort study.Am J Kidney Dis. 2015 Nov;66(5):775-82. doi: 10.1053/j.ajkd.2015.05.012. Epub 2015 Jun 26. Am J Kidney Dis. 2015. PMID: 26123862
-
Deprescribing in a family health team: a study of chronic proton pump inhibitor use.J Prim Health Care. 2016 Jun;8(2):164-71. doi: 10.1071/HC15946. J Prim Health Care. 2016. PMID: 27477559
-
Proton Pump Inhibitors and the Kidney: Implications of Current Evidence for Clinical Practice and When and How to Deprescribe.Am J Kidney Dis. 2020 Apr;75(4):497-507. doi: 10.1053/j.ajkd.2019.07.012. Epub 2019 Oct 10. Am J Kidney Dis. 2020. PMID: 31606235 Review.
Cited by
-
Approaches to Deprescribing Proton Pump Inhibitors in Clinical Practice: A Systematic Review.J Clin Med. 2024 Oct 21;13(20):6283. doi: 10.3390/jcm13206283. J Clin Med. 2024. PMID: 39458232 Free PMC article. Review.
-
Medication Deprescribing in Patients Receiving Hemodialysis: A Prospective Controlled Quality Improvement Study.Kidney Med. 2024 Mar 20;6(5):100810. doi: 10.1016/j.xkme.2024.100810. eCollection 2024 May. Kidney Med. 2024. PMID: 38628463 Free PMC article.
-
Proton Pump Inhibitors Use in Kidney Transplant Recipients: A Population-Based Study.Can J Kidney Health Dis. 2024 Feb 12;11:20543581241228723. doi: 10.1177/20543581241228723. eCollection 2024. Can J Kidney Health Dis. 2024. PMID: 38356921 Free PMC article.
-
Appropriateness of Antiplatelet Therapy and Proton Pump Inhibitor Prescribing in End-Stage Kidney Disease: A Retrospective Quality Investigation Study.Can J Kidney Health Dis. 2025 Jan 6;12:20543581241312618. doi: 10.1177/20543581241312618. eCollection 2025. Can J Kidney Health Dis. 2025. PMID: 39764378 Free PMC article.
References
-
- Bolus NE, Farrell MB, Zimmerman J. Abdominal Imaging 2017: Quality, Safety, and Dose Optimization. Reston, VA: Society of Nuclear Medicine & Molecular Imaging; 2017.
-
- Nehra AK, Alexander JA, Loftus CG, Nehra V. Proton pump inhibitors: review of emerging concerns. Mayo Clin Proc. 2018;93(2):240-246. - PubMed
LinkOut - more resources
Full Text Sources
