

Right-to-left shunts in unexplained syncope: an age- and sex-matched case-control study
- PMID: 35782252
- PMCID: PMC9246723
- DOI: 10.21037/qims-21-1060
Right-to-left shunts in unexplained syncope: an age- and sex-matched case-control study
Abstract
Background: Syncope is common, but there is no clear cause for half of the patients diagnosed with syncope. Although suspected, there is limited evidence that right-to-left shunt (RLS) is related to syncope. This matched case-control study investigated the association between RLS (exposure) and unexplained syncope (outcome).
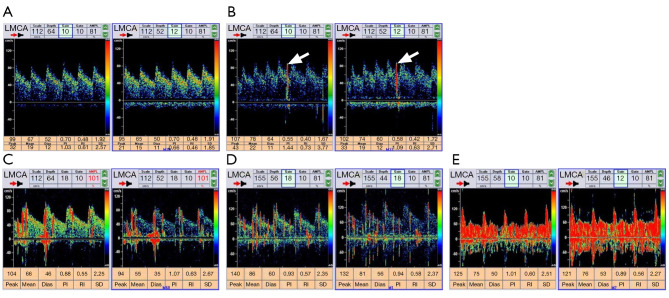
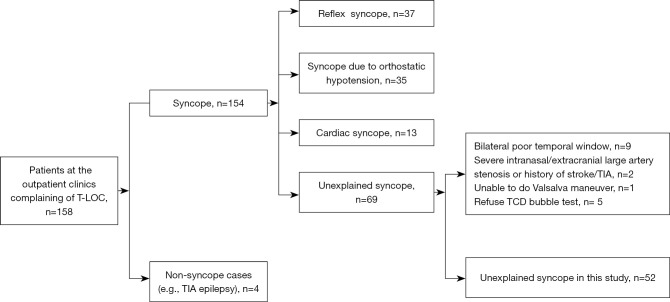
Methods: Consecutive unexplained syncope cases, together with age- and gender-matched controls who did not have syncope were recruited from 2009 to 2010 in the first affiliated hospital of Nanjing Medical University. A transcranial Doppler ultrasonography bubble test was applied for the ascertainment of RLS. The degree of RLS was categorized into grades 0 to 4 according to the number of microemboli, which were no shunt, <10 microbubbles (MB), 11-25 MB, >25 MB single spots pattern, and MB in a shower/curtain pattern, respectively. Cerebral small vessel diseases (SVD), including white matter hyperintensity, lacunes, and enlarged perivascular spaces, were rated on Magnetic resonance imaging. Conditional logistic regression was used to examine the association between RLS and unexplained syncope.
Results: A total of 52 cases and 52 age- and gender-matched controls were recruited. Among the 52 cases, 4 patients had a history of migraine. Among the 104 participants, 68 had no RLS; 13, 4, 7, and 12 presented with <10, 11-25, >25, and shower/curtain MB, respectively. The incidence of any RLS (Grade 1-4) was 48.1% (25/52) in cases and 21.2% (11/52) in controls (P=0.004). Conditional logistic regression showed an association between RLS and unexplained syncope [odds ratio (OR) =1.988; 95% confidence interval (CI): 1.233 to 3.205; P=0.005] adjusting for SVD burden. Further analysis revealed a large OR between severe RLS (Grade 3-4) and unexplained syncope (OR =8.699; P=0.006). Furthermore, SVD burden was shown to be associated with syncope.
Conclusions: This matched case-control study showed a significant association between RLS and unexplained syncope, independent of cerebral SVD. Prospective studies are needed to confirm the causal relationship.
Keywords: Right-to-left shunt (RLS); microbubble; syncope.
2022 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-21-1060/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Task Force for the Diagnosis and Management of Syncope. European Society of Cardiology (ESC) ; European Heart Rhythm Association (EHRA); Heart Failure Association (HFA); Heart Rhythm Society (HRS), Moya A, et al. Guidelines for the diagnosis and management of syncope (version 2009). Eur Heart J 2009;30:2631-71. 10.1093/eurheartj/ehp298 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous