

Tissue-engineered composite tracheal grafts create mechanically stable and biocompatible airway replacements
- PMID: 35782992
- PMCID: PMC9243572
- DOI: 10.1177/20417314221108791
Tissue-engineered composite tracheal grafts create mechanically stable and biocompatible airway replacements
Abstract
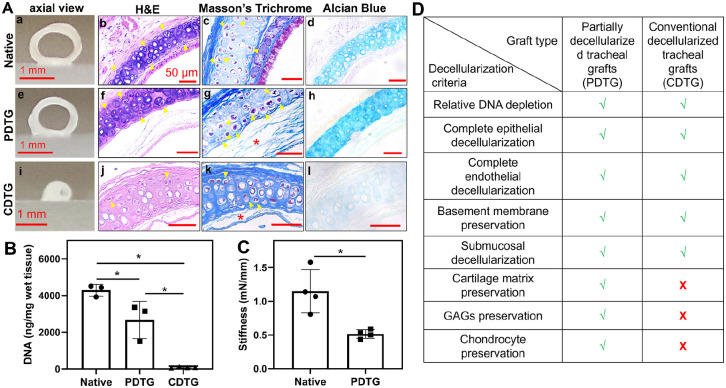
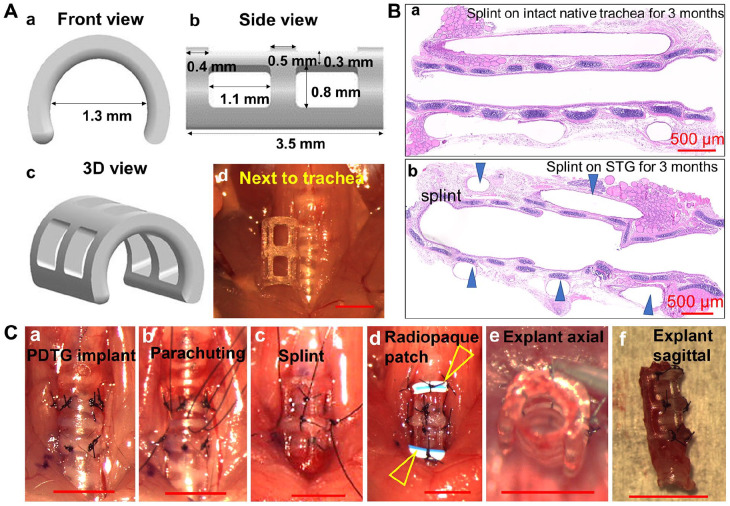
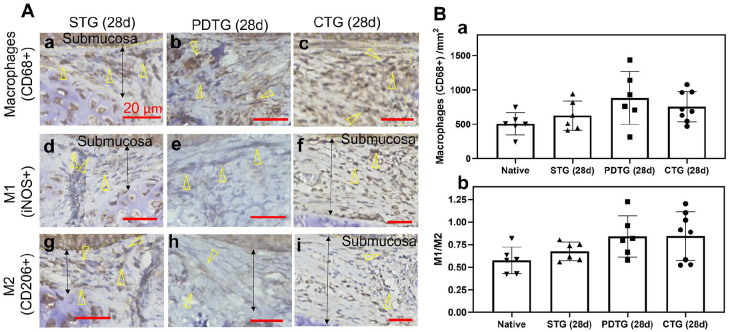
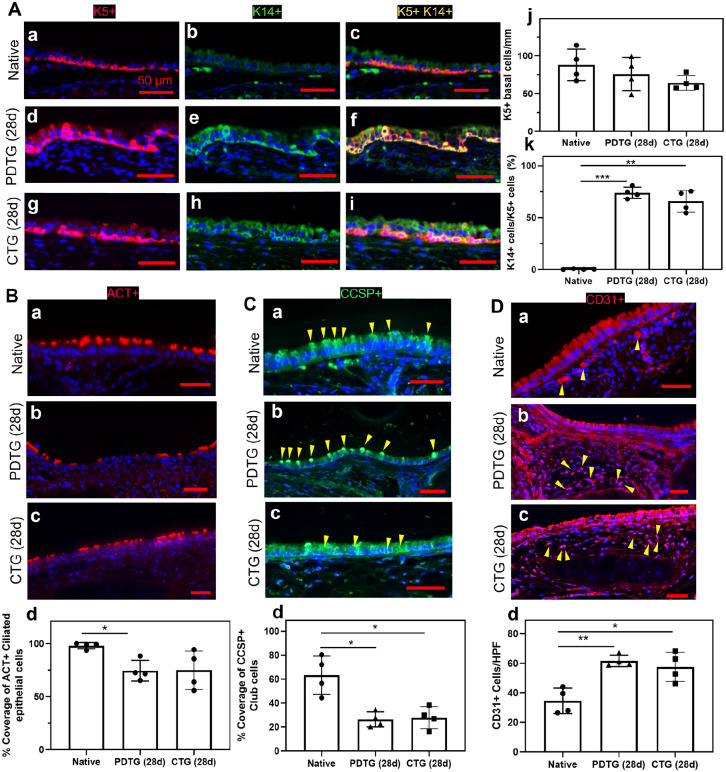
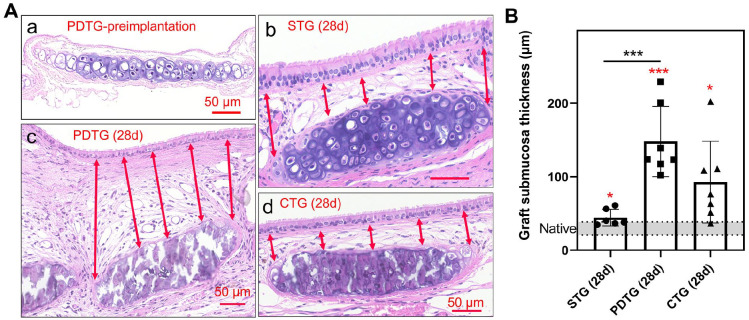
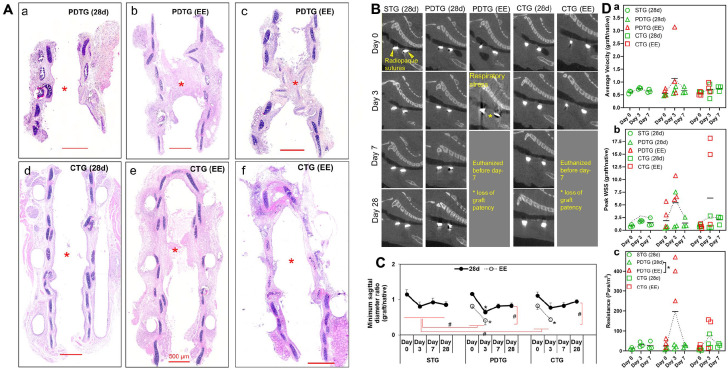
We tested composite tracheal grafts (CTG) composed of a partially decellularized tracheal graft (PDTG) combined with a 3-dimensional (3D)-printed airway splint for use in long-segment airway reconstruction. CTG is designed to recapitulate the 3D extracellular matrix of the trachea with stable mechanical properties imparted from the extraluminal airway splint. We performed segmental orthotopic tracheal replacement in a mouse microsurgical model. MicroCT was used to measure graft patency. Tracheal neotissue formation was quantified histologically. Airflow dynamic properties were analyzed using computational fluid dynamics. We found that CTG are easily implanted and did not result in vascular erosion, tracheal injury, or inflammation. Graft epithelialization and endothelialization were comparable with CTG to control. Tracheal collapse was absent with CTG. Composite tracheal scaffolds combine biocompatible synthetic support with PDTG, supporting the regeneration of host epithelium while maintaining graft structure.
Keywords: 3D-printed splint; Composite tracheal graft; partially decellularized tracheal scaffold; tissue regeneration; tracheal collapse.
© The Author(s) 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Kolb F, Simon F, Gaudin R, et al. 4-Year follow-up in a child with a total autologous tracheal replacement. New Engl J Med 2018; 378: 1355–1357. - PubMed
-
- Delaere P, Lerut T, Van Raemdonck D. Tracheal transplantation: state of the art and key role of blood supply in its success. Thorac Surg Clin 2018; 28: 337–345. - PubMed
-
- Hodde JP, Badylak SF, Brightman AO, et al. Glycosaminoglycan content of small intestinal submucosa: a bioscaffold for tissue replacement. Tissue Eng 1996; 2: 209–217. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
