

CT based bone mineral density as a predictor of proximal junctional fractures
- PMID: 35783005
- PMCID: PMC9240645
- DOI: 10.1016/j.xnsj.2022.100130
CT based bone mineral density as a predictor of proximal junctional fractures
Abstract
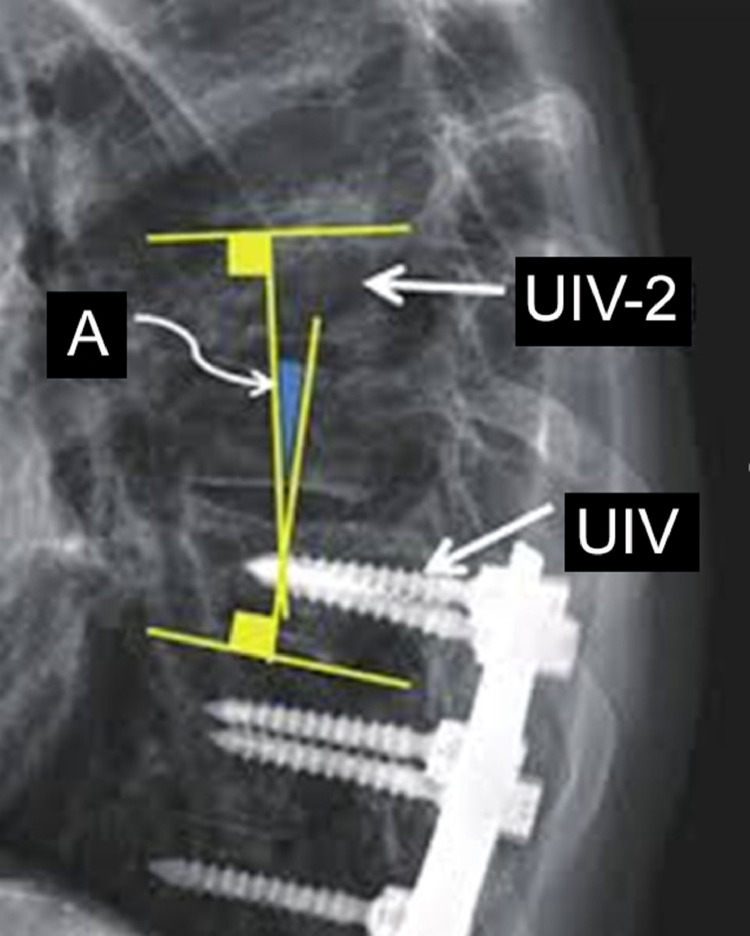
Background: Proximal junctional fractures (PJFr) can be a catastrophic complication associated with adult spinal deformity surgery. Osteoporosis can be a major risk factor for the cause of PJFr. Recent studies suggest using surrogate computed tomography (CT) scans in place of spinal dual-energy x-ray absorptiometry (DEXA) scores for bone mineral density (BMD). Investigate the feasibility of using preoperative CT based bone mineral density at upper instrumented vertebrae (UIV) and one level proximally (UIV+1) and distally (UIV-1) to predict the possibility of PJFr risk.
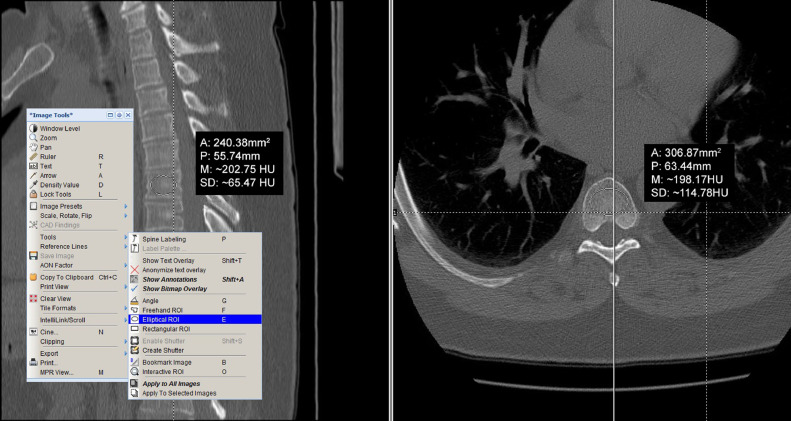
Methods: Retrospective two-academic center case-controlled study, reviewed consecutive adult spinal deformity surgeries; included constructs encompassing at least five fusion levels and fusions to pelvis. Examined demographic, surgical, and radiographic data preoperatively, postoperatively, and final follow-up. Formed groups based on type of proximal junctional deformity (PJD): Control (no PJD), proximal junctional kyphosis (PJK) and PJFr. Preoperative CT BMD values measured in Hounsfield units (HU) for sagittal and axial planes at UIV, UIV+1, and UIV-1 and compared between groups.
Results: N=92 patients. Preoperative CT scan BMD values were significantly lower in PJFr vs. control at: UIV+1 in sagittal (p=0.007), axial (p=0.02) planes; UIV sagittal (p=0.04) and axial (p=0.03) planes; and UIV-1 sagittal (p=0.05) plane. Similarly, lower CT scan BMD values noted in PJFr vs. PJK at: UIV+1 in sagittal (p=0.04) and axial (p=0.03) planes. Trend seen with lower CT scan BMD values at UIV+1 level in PJFr vs. PJK in sagittal (p=0.12) and axial (p=0.10) planes. Preoperative global sagittal imbalance measurements significantly lower in control, but comparable between PJK and PJFr.
Conclusions: Higher preoperative global sagittal imbalance with lower preoperative CT BMD values at UIV and UIV+1 vertebral body may increase the risk of proximal junctional fractures after adult spine deformity surgery. Proximal junctional hooks may supplement the pathogenesis. Readers should note the small sample size.Level of Evidence: 3.
Keywords: Bone mineral density (BMD); Computed tomography (CT) scans; Dual-energy x-ray absorptiometry (DEXA) scans; Proximal junctional fracture (PJFr); Proximal junctional kyphosis (PJK); Spine deformity surgery.
© 2022 The Authors.
Conflict of interest statement
This study was performed with the approval of SUNY Upstate Medical University IRB and The Ohio State University Wexner Medical Center IRB and in accordance with the boards’ regulations. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Similar articles
-
Sagittal Section Hounsfield Units of the Upper Instrumented Vertebrae as a Predictor of Proximal Junctional Vertebral Fractures Following Adult Spinal Deformity Surgery.Asian Spine J. 2024 Apr;18(2):209-217. doi: 10.31616/asj.2023.0339. Epub 2024 Apr 23. Asian Spine J. 2024. PMID: 38650092 Free PMC article.
-
The association between lower Hounsfield units of the upper instrumented vertebra and proximal junctional kyphosis in adult spinal deformity surgery with a minimum 2-year follow-up.Neurosurg Focus. 2020 Aug;49(2):E7. doi: 10.3171/2020.5.FOCUS20192. Neurosurg Focus. 2020. PMID: 32738804
-
Association between lower Hounsfield units and proximal junctional kyphosis and failure at the upper thoracic spine.J Neurosurg Spine. 2022 May 13;37(5):694-702. doi: 10.3171/2022.3.SPINE22197. Print 2022 Nov 1. J Neurosurg Spine. 2022. PMID: 35561697
-
The association between bone mineral density and proximal junctional kyphosis in adult spinal deformity: a systematic review and meta-analysis.J Neurosurg Spine. 2023 Apr 7;39(1):82-91. doi: 10.3171/2023.2.SPINE221101. Print 2023 Jul 1. J Neurosurg Spine. 2023. PMID: 37029673
-
Characteristics and risk factors for proximal junctional kyphosis in adult spinal deformity after correction surgery: a systematic review and meta-analysis.Neurosurg Rev. 2019 Sep;42(3):671-682. doi: 10.1007/s10143-018-1004-7. Epub 2018 Jul 7. Neurosurg Rev. 2019. PMID: 29982856
Cited by
-
Sagittal Section Hounsfield Units of the Upper Instrumented Vertebrae as a Predictor of Proximal Junctional Vertebral Fractures Following Adult Spinal Deformity Surgery.Asian Spine J. 2024 Apr;18(2):209-217. doi: 10.31616/asj.2023.0339. Epub 2024 Apr 23. Asian Spine J. 2024. PMID: 38650092 Free PMC article.
-
Hounsfield units and vertebral bone quality score for predicting mechanical complications after adult spinal deformity surgery: a systematic review and meta-analysis.Asian Spine J. 2024 Oct;18(5):719-730. doi: 10.31616/asj.2023.0402. Epub 2024 Oct 22. Asian Spine J. 2024. PMID: 39434231 Free PMC article.
-
The correlation between self-Hounsfield units and adjacent vertebral fracture after percutaneous vertebral augmentation: a retrospective cohort study.Quant Imaging Med Surg. 2024 Mar 15;14(3):2405-2414. doi: 10.21037/qims-23-1233. Epub 2024 Mar 4. Quant Imaging Med Surg. 2024. PMID: 38545073 Free PMC article.
-
The Association Between Hounsfield Units and Mechanical Failure in ASD Patients.Global Spine J. 2025 May;15(4):2218-2225. doi: 10.1177/21925682241291519. Epub 2024 Oct 13. Global Spine J. 2025. PMID: 39397242 Free PMC article.
-
Junctional Kyphosis after Correction with Long Instrumentation for Late Posttraumatic Thoracolumbar Kyphosis: Characteristics and Risk Factors.Orthop Surg. 2023 Mar;15(3):713-723. doi: 10.1111/os.13642. Epub 2023 Jan 4. Orthop Surg. 2023. PMID: 36597762 Free PMC article.
References
-
- Watanabe K, Lenke LG, Bridwell KH, Kim YJ, Koester L, Hensley M. Proximal junctional vertebral fracture in adults after spinal deformity surgery using pedicle screw constructs: analysis of morphological features. Spine (Phila Pa 1976) 2010;35(2):138–145. doi: 10.1097/BRS.0b013e3181c8f35d. PMID: 20081508. - DOI - PubMed
-
- Tamai K, Terai H, Suzuki A, et al. Risk factors for proximal junctional fracture following fusion surgery for osteoporotic vertebral collapse with delayed neurological deficits: a retrospective cohort study of 403 patients. Spine Surg Relat Res. 2018;3(2):171–177. doi: 10.22603/ssrr.2018-0068. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
