

Catheter-Based Therapies Decrease Mortality in Patients With Intermediate and High-Risk Pulmonary Embolism: Evidence From Meta-Analysis of 65,589 Patients
- PMID: 35783825
- PMCID: PMC9243366
- DOI: 10.3389/fcvm.2022.861307
Catheter-Based Therapies Decrease Mortality in Patients With Intermediate and High-Risk Pulmonary Embolism: Evidence From Meta-Analysis of 65,589 Patients
Abstract
Background: Catheter-directed therapies (CDT) are an alternative to systemic thrombolysis (ST) in pulmonary embolism (PE) patients, but the mortality benefit of CDT is unclear.
Objective: We conducted a systematic review with meta-analysis to compare the efficacy and safety of CDT and ST in intermediate-high and high-risk PE.
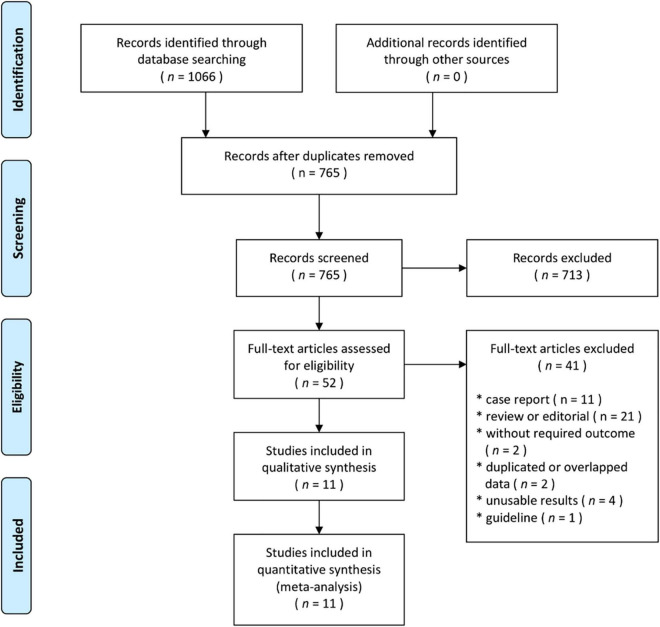
Methods: We included (P) participants, adult PE patients; (I) intervention, CDT; (C) comparison, ST; (O) outcomes, mortality, complications, in-hospital treatment, and length of hospital stay; (S) study design, randomized controlled trials (RCTs), or cohort comparing CDT and ST. The primary endpoint was 30-day mortality. Secondary outcomes included treatment-related complications including bleeding, the use of hospital resources, and length of hospital stay.
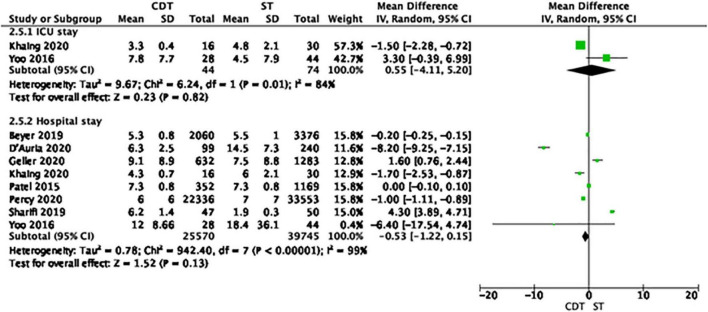
Results: Eleven studies including 65,589 patients met the inclusion criteria. Thirty-day mortality was lower in the CDT group, compared to ST group [7.3 vs. 13.6%; odds ratio (OR) = 0.51, 95% confidence interval (CI) 0.38-0.69, p < 0.001]. The rates of myocardial injury, cardiac arrest, and stroke were lower in CDT group, compared to ST group (p < 0.001 for all). The rates of any major bleeding, intracranial hemorrhage, hemoptysis, and red blood cell transfusion were lower in patients treated with CDT, compared to ST (p ≤ 0.01 for all). Extracorporeal life support was used more often in patients treated with CDT, compared to ST (0.5 vs. 0.2%, OR = 2.52, 95% CI 1.88-3.39, p < 0.001). The use of hospital resources and length of hospital stay were comparable in both groups.
Conclusion: CDT might decrease mortality in patients with intermediate-high and high-risk PE and were associated with fewer complications, including major bleeding.
Keywords: PERT; catheter-based therapies; meta-analysis; pulmonary embolism; pulmonary embolism response team.
Copyright © 2022 Pietrasik, Gąsecka, Szarpak, Pruc, Kopiec, Darocha, Banaszkiewicz, Niewada, Grabowski and Kurzyna.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Konstantinides SV, Meyer G, Galié N, Simon R, Gibbs J, Aboyans V, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Respir J. (2019) 54:1901647. 10.1183/13993003.01647-2019 - DOI - PubMed
-
- Ciampi-Dopazo JJ, Romeu-Prieto JM, Sánchez-Casado M, Romerosa B, Canabal A, Rodríguez-Blanco ML, et al. Aspiration thrombectomy for treatment of acute massive and submassive pulmonary embolism: initial single-center prospective experience. J Vasc Interv Radiol. (2018) 29:101–6. 10.1016/j.jvir.2017.08.010 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous