

Characteristics of Right Ventricular Blood Flow in Patients With Chronic Thromboembolic Pulmonary Hypertension: An Analysis With 4-Dimensional Flow Cardiovascular Magnetic Resonance Imaging
- PMID: 35783864
- PMCID: PMC9240307
- DOI: 10.3389/fcvm.2022.900301
Characteristics of Right Ventricular Blood Flow in Patients With Chronic Thromboembolic Pulmonary Hypertension: An Analysis With 4-Dimensional Flow Cardiovascular Magnetic Resonance Imaging
Abstract
Background: Blood flow is closely related to function, but currently, the relationship of right ventricular (RV) blood flow components with RV function and hemodynamics in patients with chronic thromboembolic pulmonary hypertension (CTEPH) remains unclear. Our objective is to qualify RV function with 4-dimensional flow cardiovascular magnetic resonance (4D-Flow CMR) imaging and to investigate the correlation between RV flow and hemodynamics in patients with CTEPH.
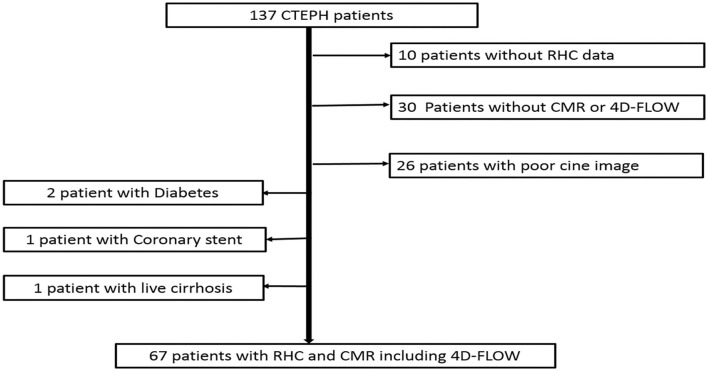
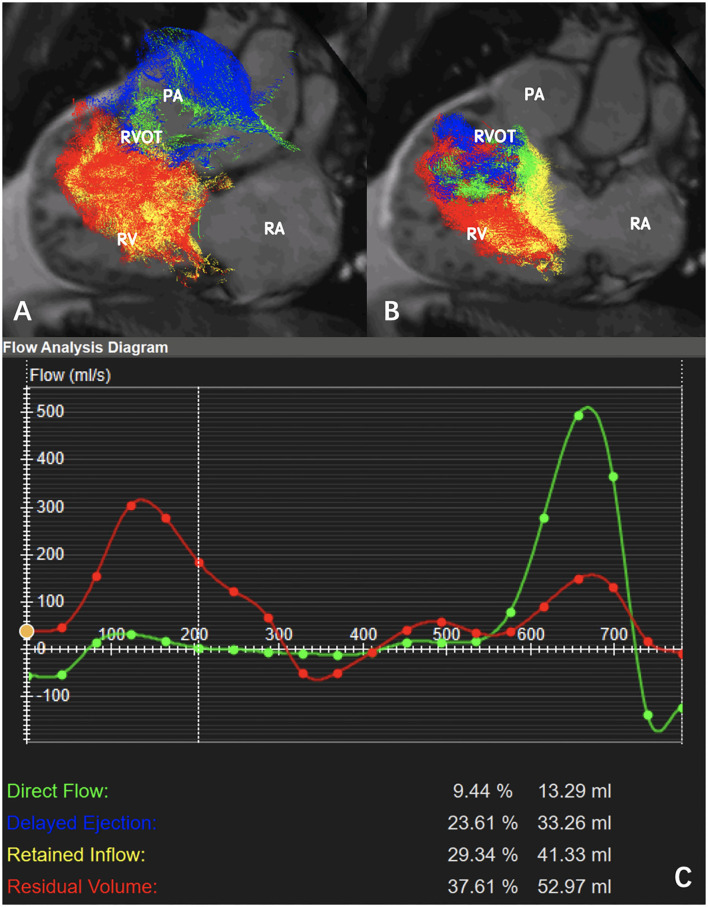
Methods: Retrospective enrollment included 67 patients with CTEPH (mean age 47.8±14.2 years, 47 men) who underwent CMR and right heart catheterization (RHC) within 2 days. RHC was used to evaluate hemodynamics. RV flow components including the percentages of direct flow (PDF), retained inflow (PRI), delayed ejection flow (PDEF), and residual volume (PRVo) were quantified on 4D-Flow sequence. RV functional metrics were determined with the CINE balanced steady-state free precession sequence. The sum of PDF and PDEF was compared with RV eject fraction (RVEF). The correlation among RV flow components, RV functional metrics and hemodynamics was analyzed with spearman correlation analysis.
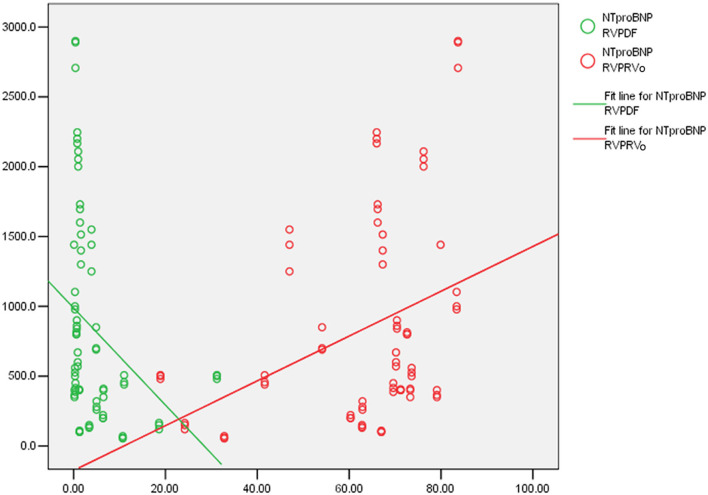
Results: The median (interquartile range) of RVEF, PDF, PDEF, PRI, and PRVo, respectively was 35.5% (18.2, 45.6%), 18% (8.4, 21.4%), 15.1% (13.5, 19.0%), 15.9% (13.8, 20.8%), and 50.6% (35.6, 60.4%). The sum of PDF and PDEF is 35.1% (24.8, 46.6%), which was similar to RVEF (z = 0.58, p = 0.561). PDF negatively correlated with right ventricular end-systolic volume index (RVESVI), right ventricular myocardial mass index (RVMI) and right ventricular global longitudinal strain (r = -0.61, -0.65, -0.64, p < 0.001). PRVo positively correlated with RVESVI and RVMI (r = 0.50, 0.58, p < 0.001). PDF negatively correlated with pulmonary vascular resistance (PVR) (r = -0.72, p < 0.001) while it positively correlated with cardiac output (CO) and cardiac index (CI) (r = 0.64 & 0.52, p < 0.001). PRVo positively correlated with mean pulmonary pressure and PVR (r = 0.57&0.54, p < 0.001). Total five patients died in the perioperative period. RVEF in the deceased patients was similar to survivors (z = -1.163, p = 0.092). In comparison with the survivors, RVPDF in the deceased patients significantly reduced (z = -2.158, p = 0.029) while RVPDEF, RVPRI, and RVPRVo in deceased patients were similar to survivors.
Conclusion: 4D-Flow CMR can provide simultaneous quantification of RV function and hemodynamics in the assessment of CTEPH without breath-holding. The reduced PDF and increased PRVo were the main characteristics of RV flow in CTEPH.
Keywords: 4-dimensional flow; cardiovascular magnetic resonance imaging; chronic thromboembolic pulmonary hypertension; hemodynamics; right ventricular function.
Copyright © 2022 Xu, Sun, Tao, Wang, Zhen, Liu, An, Xie and Liu.
Conflict of interest statement
JA was employed by Siemens Shenzhen Magnetic Resonance Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials