

Sodium Glucose Cotransporter-2 Inhibitor Protects Against Diabetic Neuropathy and Nephropathy in Modestly Controlled Type 2 Diabetes: Follow-Up Study
- PMID: 35784562
- PMCID: PMC9247156
- DOI: 10.3389/fendo.2022.864332
Sodium Glucose Cotransporter-2 Inhibitor Protects Against Diabetic Neuropathy and Nephropathy in Modestly Controlled Type 2 Diabetes: Follow-Up Study
Abstract
Aims: This three-year follow-up study aimed to elucidate whether sodium-glucose cotransporter-2 inhibitors (SGLT2is) have any protection against diabetic neuropathy and nephropathy in patients with type 2 diabetes via reducing variability in glycemia and extraglycemic factors or their averages.
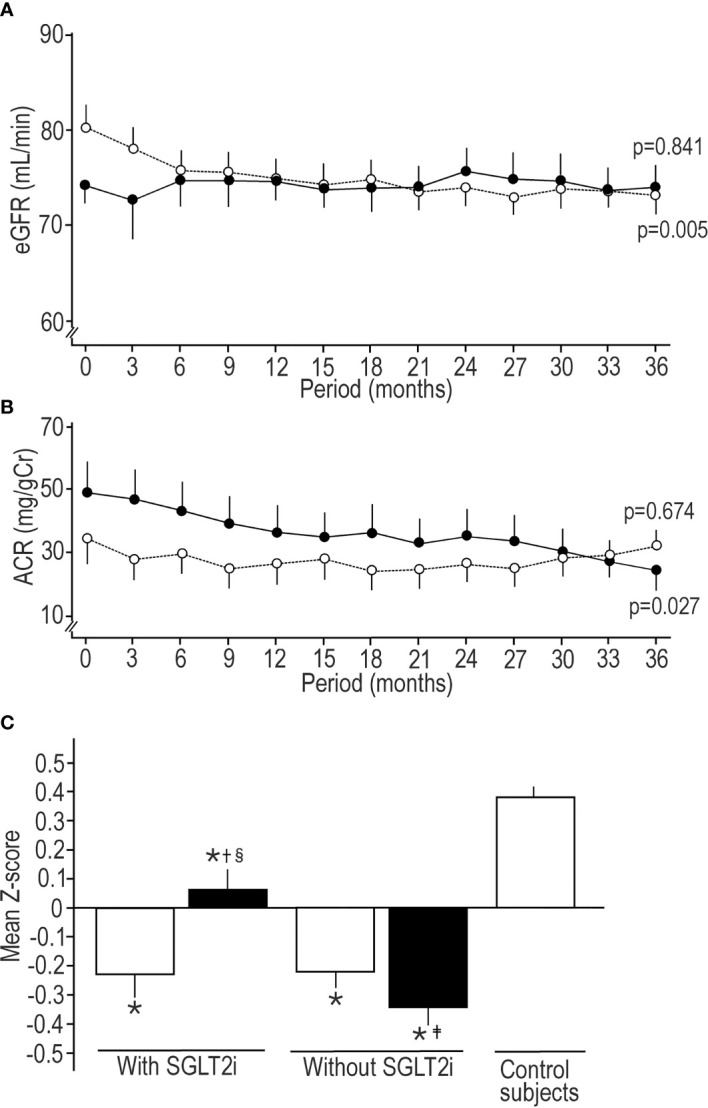
Methods: Two type 2 diabetic cohorts of 40 and 73 patients treated with or without SGLT2i along with 60 control subjects were recruited. Two diabetic cohorts matched for HbA1c levels and oral hypoglycemic agents other than SGLT2is underwent glycemic control with or without SGLT2is more than two years. The urinary albumin to creatinine ratio (ACR), estimated glomerular filtration rate (eGFR) every 3 months and neuropathy outcome measures and mean Z-score of 8 neurophysiological tests were determined at the baseline and endpoint. Glycemic variability, evaluated by the coefficient of variation of monthly measured HbA1c levels and casual postprandial plasma glucose (CPPG), and coefficient of variation and average of extraglycemic parameters in diabetic cohorts were determined.
Results: The glycemic variability and variability of some extraglycemic factors in SGLT2i cohort were smaller than those in non-SGLT2i cohort. However, only smaller coefficient of variation of HbA1c improved some neuropathy outcome measures, and ameliorated eGFR decline. SGLT2i improved the Z-score of neurophysiological tests. The optimized changes in the blood pressure, HDL-cholesterol and uric acid by SGLT2i led to neurological and renal protection. SGLT2i decreased the prevalence of nephropathy significantly and the prevalence of neuropathy insignificantly.
Conclusion: Over 3 years period, SGLT2i significantly improved some neuropathy outcome measures, mean Z-score of 8 neurophysiological tests, and attenuated nephropathy in modestly controlled type 2 diabetes by reducing glycemic variability and mean nonglycemic factors of diabetic microvascular complication.
Keywords: SGLT2i; diabetic microvascular complication; extraglycemic factors; glycemic variability; modest glycemic control; protection against neuropathy and nephropathy; type 2 diabetes.
Copyright © 2022 Ishibashi, Kosaka and Tavakoli.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Improvement in Neuropathy Outcomes With Normalizing HbA1c in Patients With Type 2 Diabetes.Diabetes Care. 2019 Jan;42(1):110-118. doi: 10.2337/dc18-1560. Epub 2018 Nov 19. Diabetes Care. 2019. PMID: 30455338
-
Blood pressure after treatment with sodium-glucose cotransporter 2 inhibitors influences renal composite outcome: Analysis using propensity score-matched models.J Diabetes Investig. 2021 Jan;12(1):74-81. doi: 10.1111/jdi.13318. Epub 2020 Jul 10. J Diabetes Investig. 2021. PMID: 32506833 Free PMC article.
-
Effects of sodium-glucose cotransporter 2 inhibitors on renal risk factors in patients with abnormal glucose metabolism: a meta-analysis of randomized controlled trials.Eur J Clin Pharmacol. 2023 Jun;79(6):859-871. doi: 10.1007/s00228-023-03490-8. Epub 2023 Apr 25. Eur J Clin Pharmacol. 2023. PMID: 37097298
-
Renal Protection and Safety of Sodium-glucose Cotransporter-2 Inhibitors in Chronic Kidney Disease.Curr Pharm Des. 2023;29(21):1659-1670. doi: 10.2174/1381612829666230804103643. Curr Pharm Des. 2023. PMID: 37537933
-
Sodium-glucose cotransporter 2 inhibitors as an add-on therapy to insulin for type 1 diabetes mellitus: Meta-analysis of randomized controlled trials.Acta Diabetol. 2021 Jul;58(7):869-880. doi: 10.1007/s00592-021-01686-x. Epub 2021 Mar 2. Acta Diabetol. 2021. PMID: 33651228 Free PMC article.
Cited by
-
Dapagliflozin combined with methylcobalamin in the treatment of type 2 diabetes mellitus with peripheral neuropathy: a systematic review and meta-analysis.Front Endocrinol (Lausanne). 2025 Jun 19;16:1514783. doi: 10.3389/fendo.2025.1514783. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40612436 Free PMC article.
-
The Potential Impact of SGLT2-I in Diabetic Foot Prevention: Promising Pathophysiologic Implications, State of the Art, and Future Perspectives-A Narrative Review.Medicina (Kaunas). 2024 Nov 1;60(11):1796. doi: 10.3390/medicina60111796. Medicina (Kaunas). 2024. PMID: 39596981 Free PMC article. Review.
-
Novel glucose-lowering agents that benefit diabetic foot: icing on the cake.Front Endocrinol (Lausanne). 2025 Jul 2;16:1581403. doi: 10.3389/fendo.2025.1581403. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40671916 Free PMC article. Review.
-
The Impact of SGLT-2 Inhibitors on Hydroxyl Radical Markers and Diabetic Neuropathy: A Short-Term Clinical Study.Antioxidants (Basel). 2025 Feb 28;14(3):289. doi: 10.3390/antiox14030289. Antioxidants (Basel). 2025. PMID: 40227261 Free PMC article.
-
Understanding the heterogeneity and dysfunction of HDL in chronic kidney disease: insights from recent reviews.BMC Nephrol. 2024 Nov 7;25(1):400. doi: 10.1186/s12882-024-03808-3. BMC Nephrol. 2024. PMID: 39511510 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous