

Liquid First Is "Solid" in Naïve Non-Small Cell Lung Cancer Patients: Faster Turnaround Time With High Concordance to Solid Next-Generation Sequencing
- PMID: 35785173
- PMCID: PMC9242672
- DOI: 10.3389/fonc.2022.912801
Liquid First Is "Solid" in Naïve Non-Small Cell Lung Cancer Patients: Faster Turnaround Time With High Concordance to Solid Next-Generation Sequencing
Abstract
Purpose: Molecular profiling is crucial in naïve non-small cell lung cancer (NSCLC). While tissue-based analysis is challenged by turnaround time and scarcity of tissue, there is increasing demand for liquid biopsy. We aimed to analyze the use of upfront liquid biopsy as a molecular profiling approach.
Methods: This retrospective multicenter, non-interventional study compared findings and turnaround times of liquid vs. standard-of-care (SOC) tissue-biopsy molecular profiling. The study included naïve advanced NSCLC patients with available liquid biopsy (Guardant360 CDx).
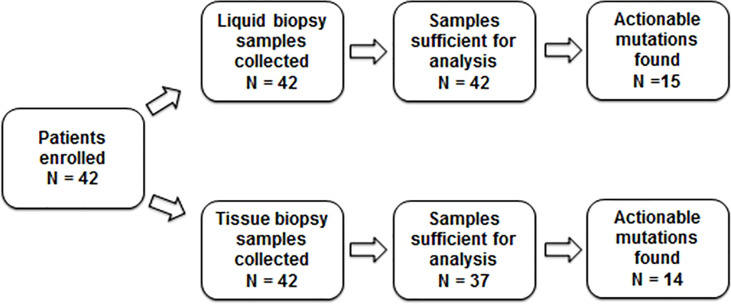
Results: A total of 42 consecutive patients (60% men; median age, 69.5 [39-87] years; 86% stage IV NSCLC) were identified between September 2017 and December 2020. Liquid-biopsy analysis provided results for all 42 patients, whereas the tissue-based analysis failed in 5 (12%) patients due to insufficient tumor samples. In 17 patients, 18 actionable driver mutations were identified. Eleven mutations were detected by both approaches (i.e., concordance of 61%), 4 only by liquid biopsy and 3 only by tissue biopsy. The median time from the molecular request to receiving the molecular solid report on the last biomarker was 21 (range: 5-66) days, whereas the median time from blood draw to the liquid-biopsy results was 10.5 (7-19) days. The median time between the availability of liquid-biopsy findings and that of the last biomarker was 5 days. Treatment changes following the liquid-biopsy results were observed in 3 (7%) patients.
Conclusion: Performing liquid-biopsy upfront is feasible and accurate and allows a shorter time for treatment in NSCLC, especially when tumor tissue is scarce.
Keywords: circulating tumor DNA (ctDNA); driver mutation; liquid biopsy; non-small cell lung carcinoma (NSCLC); turnaround time (TAT).
Copyright © 2022 Sehayek, Kian, Onn, Stoff, Sorotsky, Zemel, Bar, Dudnik, Nechushtan, Rottenberg, Soussan-Gutman, Dvir, Roisman and Peled.
Conflict of interest statement
AD and LS-G are employed and are shareholders at Rhenium Oncotest Ltd. NP declares advisor and honorarium from and research with AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, Foundation Medicine, Guardant360, Merck, MSD, Novartis, NovellusDx, Pfizer, Roche, and Takeda. YR declares a speakers bureau from MSD, AZD, Roche, Dexcel, Medison, and Novartis and is a consultant for MSD and Takeda. JB declares research funding (for the institute) and advisor fees from MSD, AstraZeneca, Pfizer, Takeda, AbbVie, Roche, Novartis, and Merck Serono and share options from Causalis. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Lindeman NI, Cagle PT, Aisner DL, Arcila ME, Beasley MB, Bernicker EH, et al. . Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment With Targeted Tyrosine Kinase Inhibitors: Guideline From the College of American Pathologists, the International Association for the Study of Lung Cancer, and the Association for Molecular Pathology. J Thorac Oncol (2018) 13(3):323–58. doi: 10.5858/arpa.2017-0388-CP - DOI - PubMed
LinkOut - more resources
Full Text Sources