

Hematologic abnormalities in Aicardi Goutières Syndrome
- PMID: 35786528
- PMCID: PMC9357135
- DOI: 10.1016/j.ymgme.2022.06.003
Hematologic abnormalities in Aicardi Goutières Syndrome
Abstract
Background: Because of the broad clinical spectrum, heritable autoinflammatory diseases present a management and therapeutic challenge. The most common genetic interferonopathy, Aicardi Goutières Syndrome (AGS), is associated with early onset neurologic disability and systemic inflammation. The chronic inflammation of AGS is the result of dysregulation of interferon (IFN) expression by one of nine genes within converging pathways. While each AGS subtype shares common features, distinct patterns of severity and potential for systemic complications amongst the genotypes are emerging. Multilineage cytopenias are a potentially serious, but poorly understood, complication of AGS. As immunomodulatory treatment options are developed, it is important to characterize the role of the disease versus treatment in hematologic abnormalities. This will allow for better understanding and management of cytopenia.
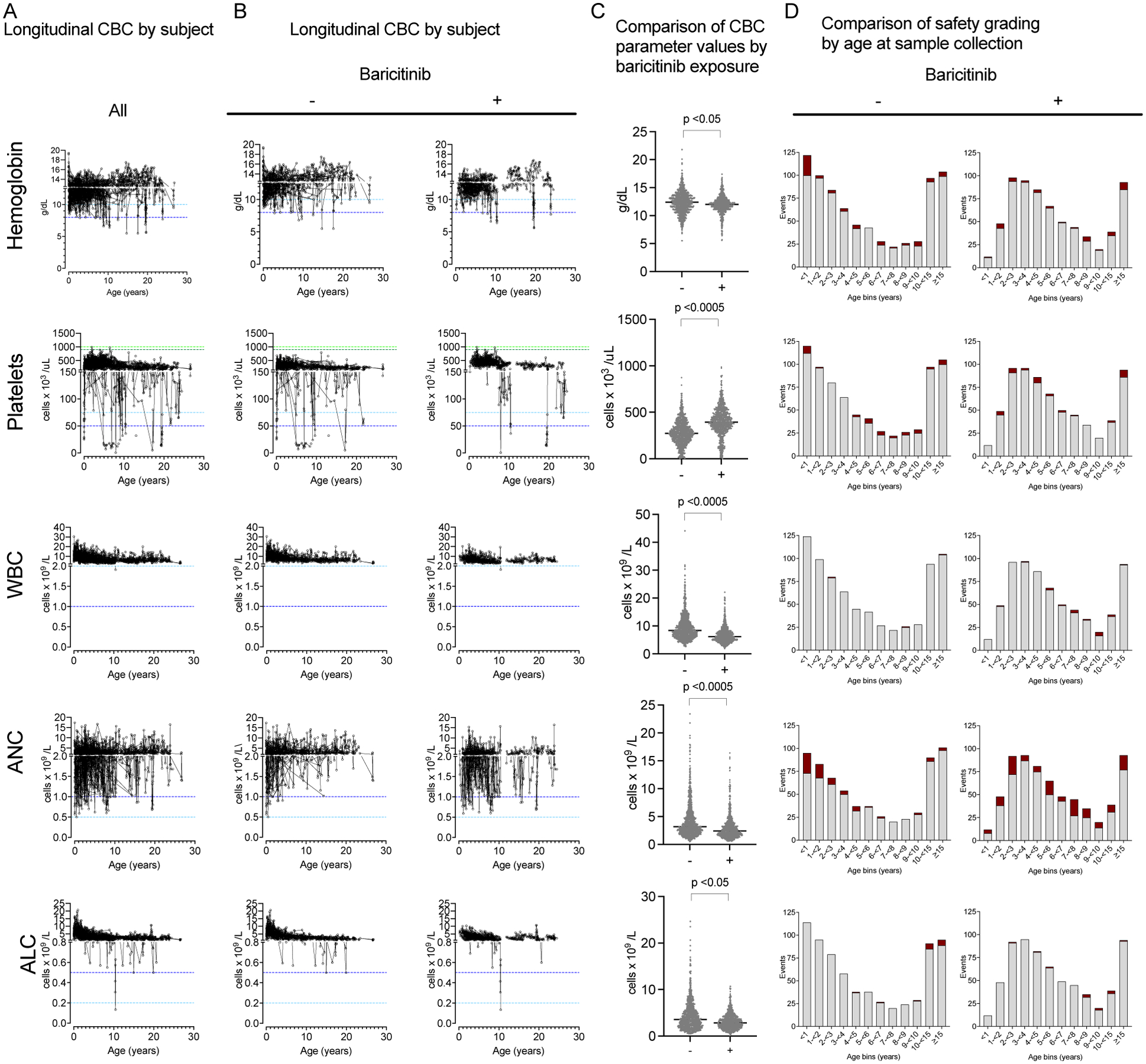
Methods: In total, 142 individuals with molecularly-confirmed AGS were included. Information on genotype, demographics, and all available hematologic laboratory values were collected from existing medical records. As part of a clinical trial, a subset of this cohort (n = 52) were treated with a janus kinase inhibitor (baricitinib), and both pre- and post-treatment values were included. Abnormal values were graded based on Common Terminology Criteria for Adverse Events (CTCAE v5.0), supplemented with grading definitions for thrombocytosis, and were compared across genotypes and baricitinib exposure.
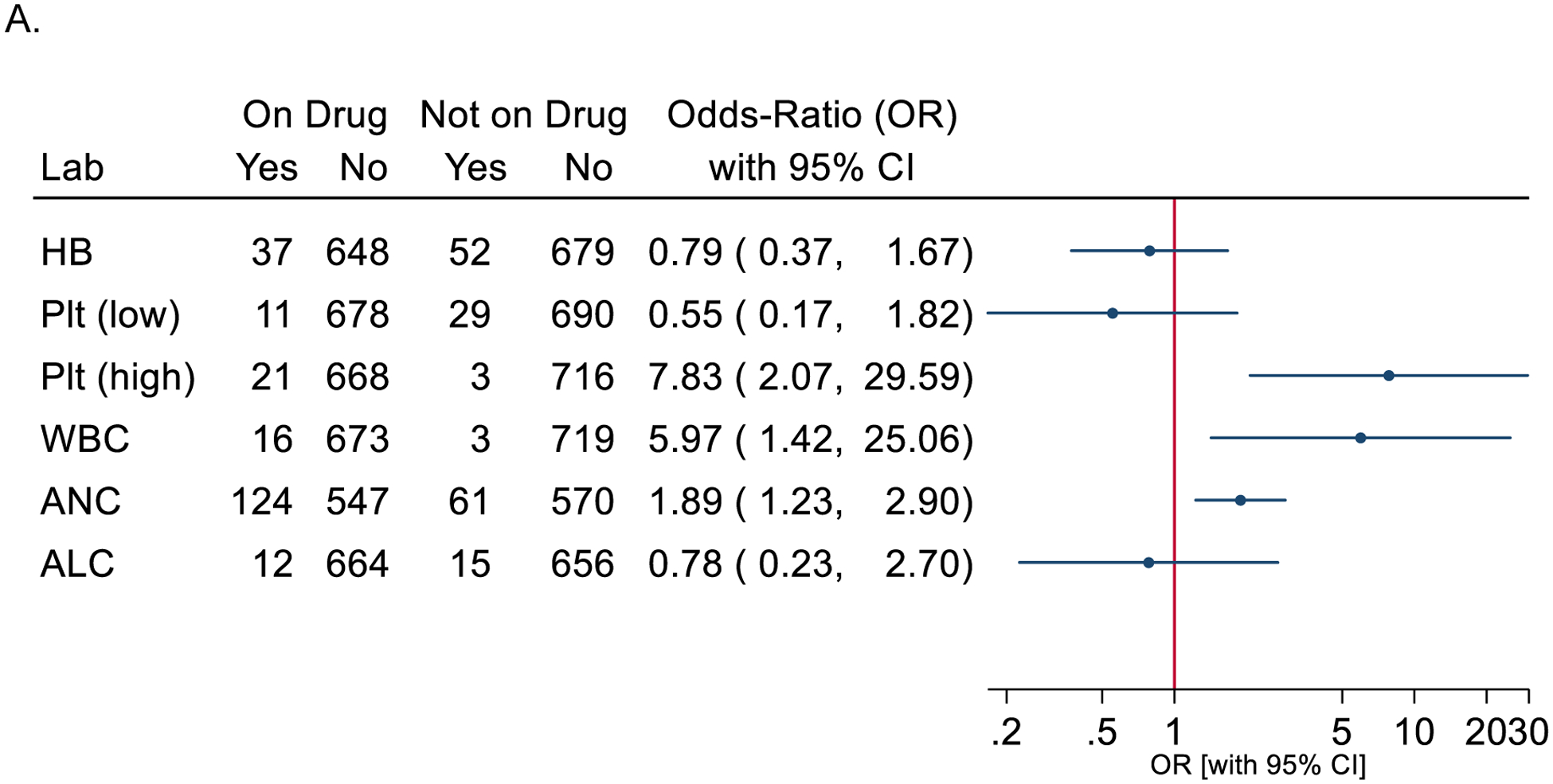
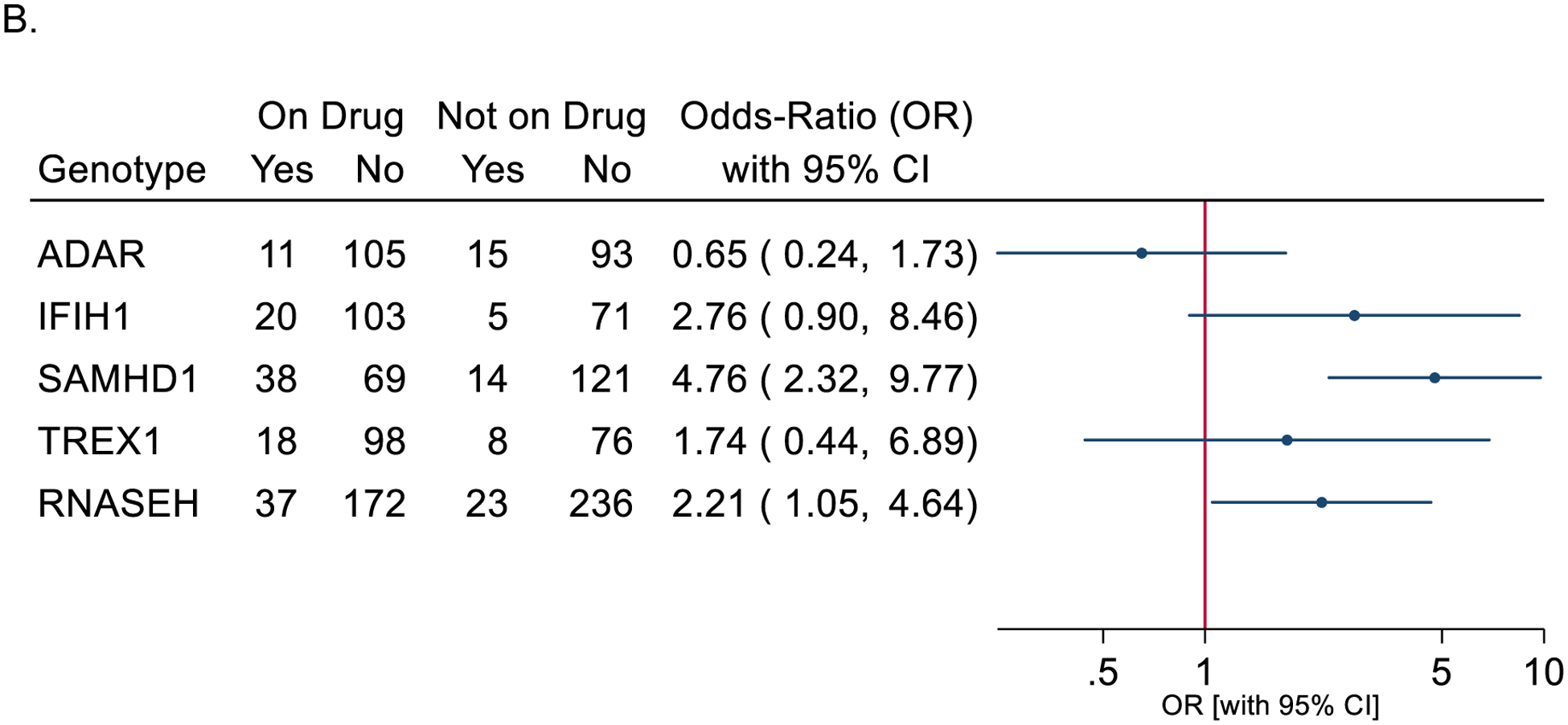
Results: In total, 11,184 laboratory values were collected over a median of 2.54 years per subject (range 0-22.68 years). To reduce bias from repeated sampling within a limited timeframe, laboratory results were restricted to the most abnormal value within a month (n = 8485). The most common abnormalities were anemia (noted in 24% of subjects prior to baricitinib exposure), thrombocytopenia (9%), and neutropenia (30%). Neutropenia was most common in the SAMHD1 cohort and increased with baricitinib exposure (38/69 measurements on baricitinib versus 14/121 while not on baricitinib). Having an abnormality prior to treatment was associated with having an abnormality on treatment for neutropenia and thrombocytopenia.
Conclusion: By collecting available laboratory data throughout the lifespan, we were able to identify novel patterns of hematologic abnormalities in AGS. We found that AGS results in multilineage cytopenias not limited to the neonatal period. Neutropenia, anemia, and thrombocytopenia were common. Moderate-severe graded events of neutropenia, anemia, and leukopenia were more common on baricitinib, but rarely of clinical consequence. Based on these results, we would recommend careful monitoring of hematologic parameters of children affected by AGS throughout the lifespan, especially while on therapy, and consideration of AGS as a potential differential diagnosis in children with neurologic impairment of unclear etiology with hematologic abnormalities. Trial registration ClinicalTrials.gov Identifier: NCT01724580 ClinicalTrials.gov Identifier: NCT03921554.
Keywords: Genetic disorder; Hematology; Janus kinase inhibitor; Leukodystrophy.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
-
- Uggenti C, Lepelley A, Depp M, et al. cGAS-mediated induction of type I interferon due to inborn errors of histone pre-mRNA processing. Nat Genet 2020;52:1364–1372. - PubMed
-
- Livingston JH, Crow YJ. Neurologic Phenotypes Associated with Mutations in TREX1, RNASEH2A, RNASEH2B, RNASEH2C, SAMHD1, ADAR1, and IFIH1: Aicardi-Goutieres Syndrome and Beyond. Neuropediatrics 2016;47:355–360. - PubMed
Publication types
MeSH terms
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
