

Phantom Networks: Discrepancies Between Reported And Realized Mental Health Care Access In Oregon Medicaid
- PMID: 35787079
- PMCID: PMC9876384
- DOI: 10.1377/hlthaff.2022.00052
Phantom Networks: Discrepancies Between Reported And Realized Mental Health Care Access In Oregon Medicaid
Abstract
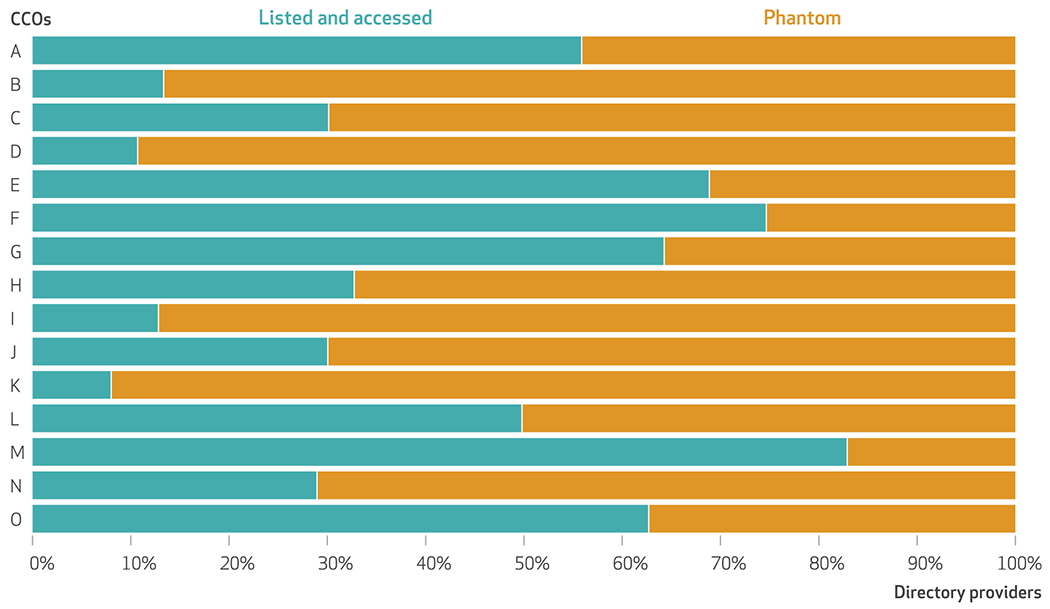
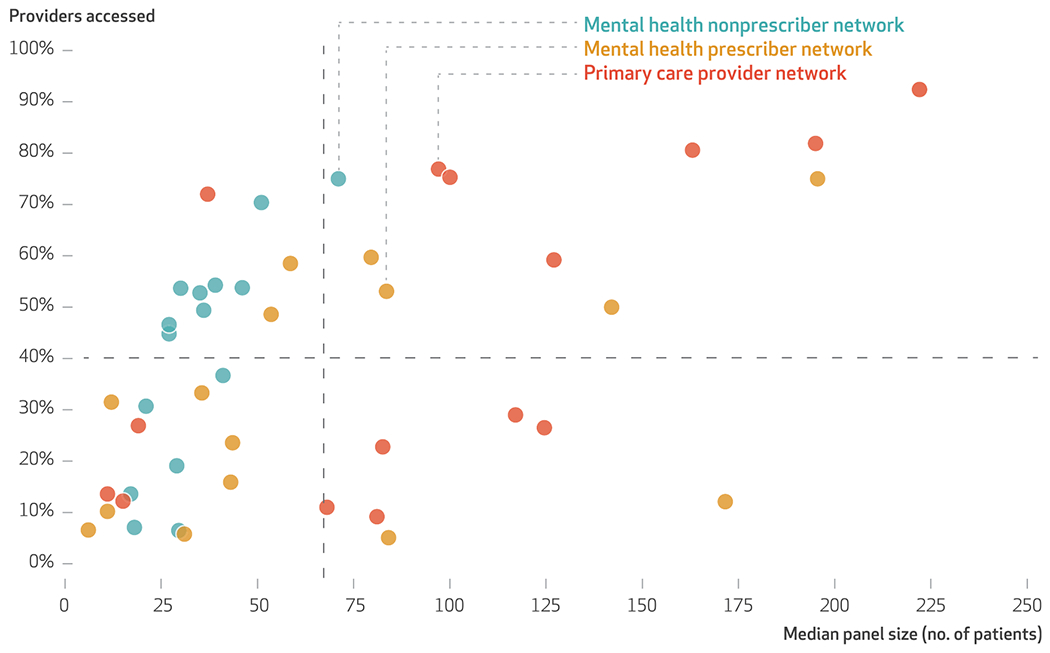
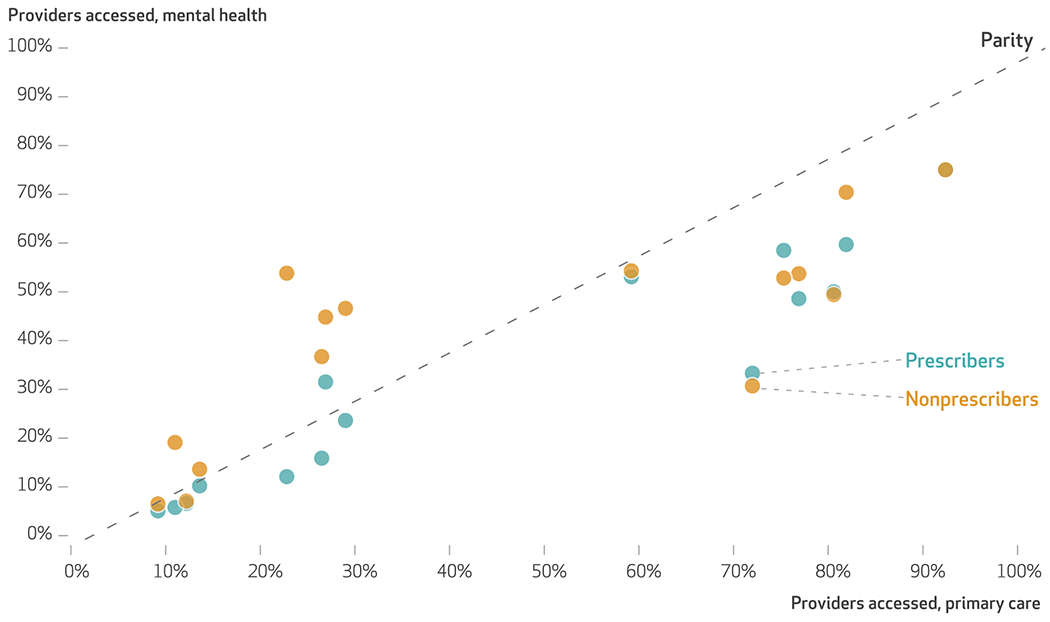
Understanding the extent to which beneficiaries can "realize" access to reported provider networks is imperative in mental health care, where there are significant unmet needs. We compared listings of providers in network directories against provider networks empirically constructed from administrative claims among members who were ages sixty-four and younger and enrolled in Oregon's Medicaid managed care organizations between January 1 and December 31, 2018. "In-network" providers were those with any medical claims filed for at least five unique Medicaid beneficiaries enrolled in a given health plan. They included primary care providers, specialty mental health prescribers, and nonprescribing mental health clinicians. Overall, 58.2 percent of network directory listings were "phantom" providers who did not see Medicaid patients, including 67.4 percent of mental health prescribers, 59.0 percent of mental health nonprescribers, and 54.0 percent of primary care providers. Significant discrepancies between the providers listed in directories and those whom enrollees can access suggest that provider network monitoring and enforcement may fall short if based on directory information.
Figures
Comment in
-
How Phantom Networks And Other Barriers Impede Progress On Mental Health Insurance Reform.Health Aff (Millwood). 2022 Jul;41(7):1023-1025. doi: 10.1377/hlthaff.2022.00541. Health Aff (Millwood). 2022. PMID: 35787083
Similar articles
-
Characteristics of Specialty Mental Health Provider Networks in Oregon Medicaid.Psychiatr Serv. 2023 Feb 1;74(2):134-141. doi: 10.1176/appi.ps.202100623. Epub 2022 Jun 30. Psychiatr Serv. 2023. PMID: 35770424 Free PMC article.
-
Rural and frontier access to mental health prescribers and nonprescribers: A geospatial analysis in Oregon Medicaid.J Rural Health. 2024 Jan;40(1):16-25. doi: 10.1111/jrh.12761. Epub 2023 Apr 23. J Rural Health. 2024. PMID: 37088967 Free PMC article.
-
Early Performance in Medicaid Accountable Care Organizations: A Comparison of Oregon and Colorado.JAMA Intern Med. 2017 Apr 1;177(4):538-545. doi: 10.1001/jamainternmed.2016.9098. JAMA Intern Med. 2017. PMID: 28192568 Free PMC article.
-
Medicaid Managed Care's Effects on Costs, Access, and Quality: An Update.Annu Rev Public Health. 2020 Apr 2;41:537-549. doi: 10.1146/annurev-publhealth-040119-094345. Annu Rev Public Health. 2020. PMID: 32237985 Review.
-
State Efforts to Regulate Provider Networks and Directories: Lessons for the Future.J Health Polit Policy Law. 2023 Dec 1;48(6):951-968. doi: 10.1215/03616878-10852610. J Health Polit Policy Law. 2023. PMID: 37497889 Review.
Cited by
-
Psychiatrist Networks In Medicare Advantage Plans Are Substantially Narrower Than In Medicaid And ACA Markets.Health Aff (Millwood). 2023 Jul;42(7):909-918. doi: 10.1377/hlthaff.2022.01547. Health Aff (Millwood). 2023. PMID: 37406238 Free PMC article.
-
Disparities in Access to Diagnostic Evaluation for Alzheimer's Disease in Individuals Dually Eligible for Medicare and Medicaid: A Modeling Study.J Alzheimers Dis. 2024;98(4):1403-1414. doi: 10.3233/JAD-231134. J Alzheimers Dis. 2024. PMID: 38517787 Free PMC article.
-
Determinants of referral network size for screening colonoscopies in the Veterans Health Administration after the implementation of the MISSION Act.Health Serv Res. 2024 Feb;59(1):e14239. doi: 10.1111/1475-6773.14239. Epub 2023 Sep 26. Health Serv Res. 2024. PMID: 37750017 Free PMC article.
-
How Specialized Are Special Needs Plans? Evidence From Provider Networks.Med Care Res Rev. 2025 Feb;82(1):58-67. doi: 10.1177/10775587241296194. Epub 2024 Nov 19. Med Care Res Rev. 2025. PMID: 39560115 Free PMC article.
-
Rural-urban differences in out-of-network treatment initiation and engagement rates for substance use disorders.Health Serv Res. 2024 Oct;59(5):e14299. doi: 10.1111/1475-6773.14299. Epub 2024 Mar 8. Health Serv Res. 2024. PMID: 38456488 Free PMC article.
References
-
- Centers for Medicare and Medicaid Services. Online provider directory review report [Internet]. Baltimore (MD): CMS; 2018. 28 Nov [cited 2022 May 19]. [Third year]. Available from: https://www.cms.gov/Medicare/Health-Plans/ManagedCareMarketing/Downloads...
-
- Adelberg M, Frakt A, Polsky D, Strollo MK. Improving provider directory accuracy: can machine-readable directories help? Am J Manag Care. 2019;25(5):241–5. - PubMed
-
- Burman A, Haeder SF. Potemkin protections: assessing provider directory accuracy and timely access for four specialties in California. J Health Polit Policy Law. 2022;47(3):319–49. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical