

Preventing Cardiac Arrest in the Pediatric Cardiac Intensive Care Unit Through Multicenter Collaboration
- PMID: 35788631
- PMCID: PMC9257678
- DOI: 10.1001/jamapediatrics.2022.2238
Preventing Cardiac Arrest in the Pediatric Cardiac Intensive Care Unit Through Multicenter Collaboration
Abstract
Importance: Preventing in-hospital cardiac arrest (IHCA) likely represents an effective strategy to improve outcomes for critically ill patients, but feasibility of IHCA prevention remains unclear.
Objective: To determine whether a low-technology cardiac arrest prevention (CAP) practice bundle decreases IHCA rate.
Design, setting, and participants: Pediatric cardiac intensive care unit (CICU) teams from the Pediatric Cardiac Critical Care Consortium (PC4) formed a collaborative learning network to implement the CAP bundle consistent with the Institute for Healthcare Improvement framework; 15 hospitals implemented the bundle voluntarily. Risk-adjusted IHCA incidence rates were analyzed across 2 time periods, 12 months (baseline) and 18 months after CAP implementation (intervention) using difference-in-differences (DID) regression to compare 15 CAP and 16 control PC4 hospitals that chose not to participate in CAP but had IHCA rates tracked in the PC4 registry. Patients deemed at high risk for IHCA, based on a priori evidence-based criteria and empirical hospital-specific criteria, were selected to receive the CAP bundle. Data were collected from July 2018 to December 2019, and data were analyzed from March to August 2020.
Interventions: CAP bundle included 5 elements developed to promote increased situational awareness and communication among bedside clinicians to recognize and mitigate deterioration in high-risk patients.
Main outcomes and measures: Risk-adjusted IHCA incidence rate across all CICU admissions (IHCA events divided by all admissions).
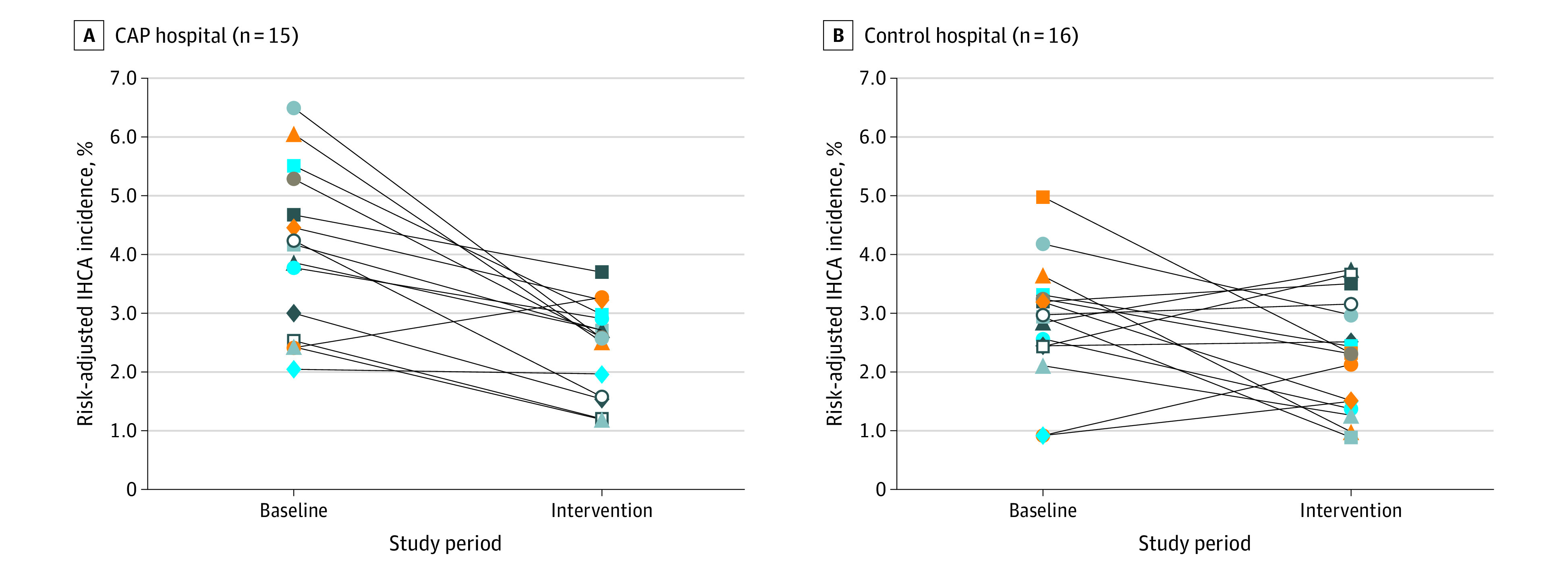
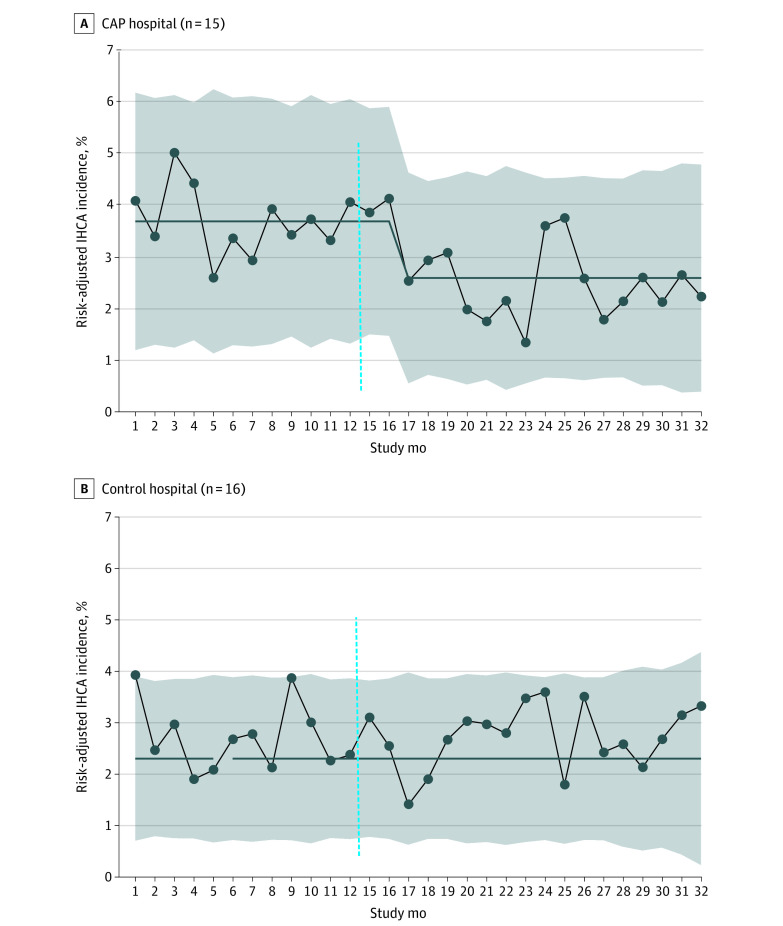
Results: The bundle was activated in 2664 of 10 510 CAP hospital admissions (25.3%); admission characteristics were similar across study periods. There was a 30% relative reduction in risk-adjusted IHCA incidence rate at CAP hospitals (intervention period: 2.6%; 95% CI, 2.2-2.9; baseline: 3.7%; 95% CI, 3.1-4.0), but no change at control hospitals (intervention period: 2.7%; 95% CI, 2.3-2.9; baseline: 2.7%; 95% CI, 2.2-3.0). DID analysis confirmed significantly reduced odds of IHCA among all admissions at CAP hospitals compared with control hospitals during the intervention period vs baseline (odds ratio, 0.72; 95% CI, 0.56-0.91; P = .01). DID odds ratios were 0.72 (95% CI, 0.53-0.98) for the surgical subgroup, 0.74 (95% CI, 0.48-1.14) for the medical subgroup, and 0.72 (95% CI, 0.50-1.03) for the high-risk admission subgroup at CAP hospitals after intervention. All-cause risk-adjusted mortality rate did not change after intervention.
Conclusions and relevance: Implementation of this CAP bundle led to significant IHCA reduction across multiple pediatric CICUs. Future studies may determine if this bundle can be effective in other critically ill populations.
Conflict of interest statement
Figures
Comment in
-
Collaboration, bundles and preventing in hospital cardiac arrests.Arch Dis Child. 2022 Dec;107(12):1121. doi: 10.1136/archdischild-2022-325088. Arch Dis Child. 2022. PMID: 36396167 No abstract available.
-
Preventing cardiac arrest in high-risk children by implementing low-cost technology independent quality improvement safety bundle.Evid Based Nurs. 2023 Jul;26(3):100. doi: 10.1136/ebnurs-2022-103617. Epub 2023 Mar 3. Evid Based Nurs. 2023. PMID: 36868825 No abstract available.
References
-
- Wolfe HA, Sutton RM, Reeder RW, et al. ; Eunice Kennedy Shriver National Institute of Child Health; Human Development Collaborative Pediatric Critical Care Research Network; Pediatric Intensive Care Quality of Cardiopulmonary Resuscitation Investigators . Functional outcomes among survivors of pediatric in-hospital cardiac arrest are associated with baseline neurologic and functional status, but not with diastolic blood pressure during CPR. Resuscitation. 2019;143:57-65. doi:10.1016/j.resuscitation.2019.08.006 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
