

[Development and validation of a prognostic model based on SEER data for patients with esophageal carcinoma after esophagectomy]
- PMID: 35790429
- PMCID: PMC9257361
- DOI: 10.12122/j.issn.1673-4254.2022.06.02
[Development and validation of a prognostic model based on SEER data for patients with esophageal carcinoma after esophagectomy]
Abstract
Objective: To develop a nomogram to predict the long-term survival of patients with esophageal cancer following esophagectomy.
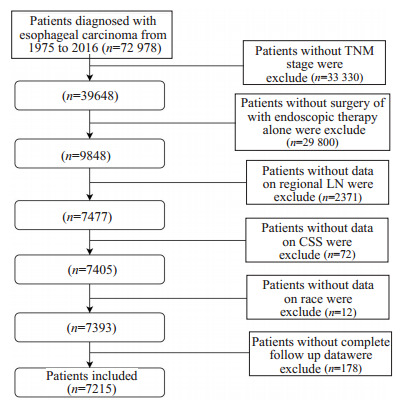
Methods: We collected the data of 7215 patients with esophageal carcinoma from the Surveillance, Epidemiology, and End Results (SEER) database during the period from 2004 and 2016. Of these patients, 5052 were allocated to the training cohort and the remaining 2163 patients to the internal validation cohort using bootstrap resampling, with another 435 patients treated in the Department of Cardiothoracic Surgery of Jinling Hospital between 2014 and 2016 serving as the external validation cohort.
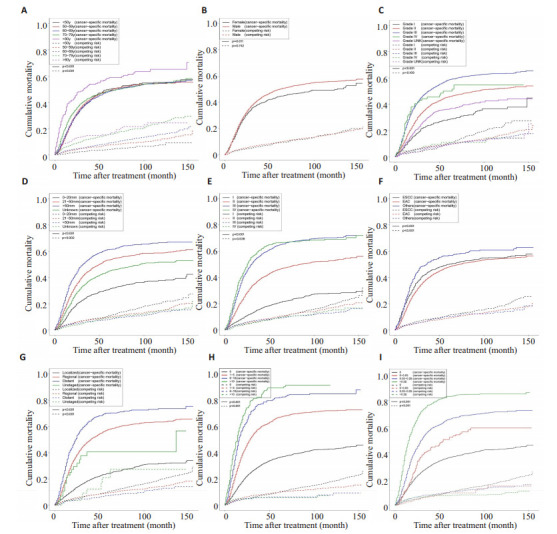
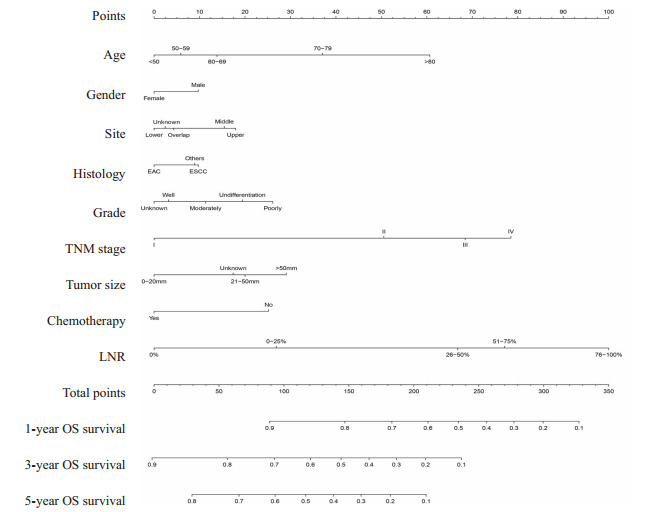
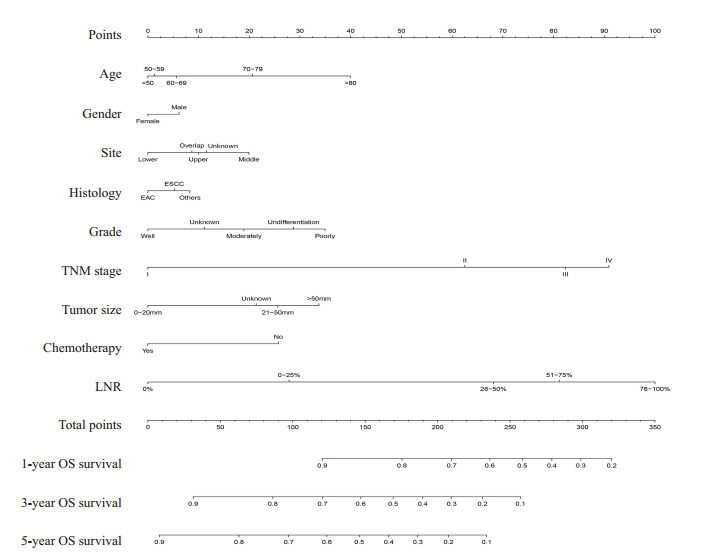
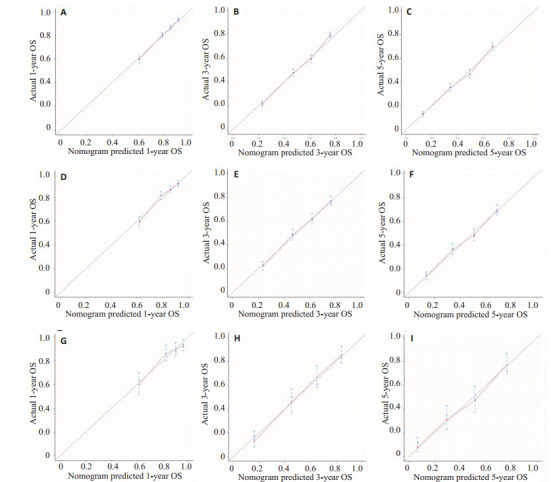
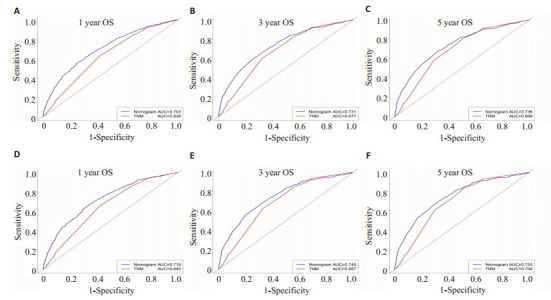
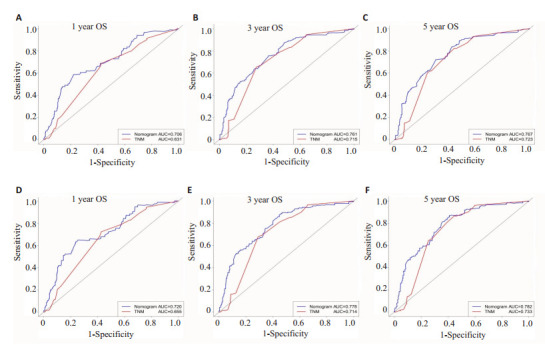
Results: In the overall cohort, the 1-, 3-, and 5-year cancer-specific mortality rates were 14.6%, 35.7% and 41.6%, respectively. Age (≥80 years vs < 50 years, P < 0.001), gender (male vs female, P < 0.001), tumor site (lower vs middle segment, P=0.013), histology (EAC vs ESCC, P=0.012), tumor grade (poorly vs well differentiated, P < 0.001), TNM stage (Ⅳ vs Ⅰ, P < 0.001), tumor size (> 50 mm vs 0-20 mm, P < 0.001), chemotherapy (yes vs no, P < 0.001), and LNR (> 0.25 vs 0, P < 0.001) were identified as independent risk factors affecting long-term survival of the patients. The nomograms established based on the model for predicting the survival probability of the patients at 1, 3 and 5 years after operation showed a C-index of 0.726 (95% CI: 0.714-0.738) for predicting the overall survival (OS) and of 0.735 (95% CI: 0.727-0.743) for cancer-specific survival (CSS) in the training cohort. In the internal validation cohort, the C-index of the nomograms was 0.752 (95% CI: 0.738-0.76) for OS and 0.804 (95% CI: 0.790-0.817) for CSS, as compared with 0.749 (95% CI: 0.736-0.767) and 0.788 (95%CI: 0.751-0.808), respectively, in the external validation cohort. The nomograms also showed a higher sensitivity than the TNM staging system for predicting long-term prognosis.
Conclusion: This prognostic model has a high prediction efficiency and can help to identify the high-risk patients with esophageal carcinoma after surgery and serve as a supplement for the current TNM staging system.
目的: 构建用于预测食管癌患者术后远期生存的列线图。
方法: 从监测、流行病学和最终结果(SEER)数据库中确定了2004~2016年7215例食管癌患者。使用自助重抽样方法,共有5052名患者被分配到训练队列,其余2163名患者被分配到内部验证队列,同时纳入2014~2016年就诊于东部战区总医院心胸外科的435名食管癌患者进行外部验证。
结果: 在整个队列中,1年、3年、5年的癌症特异性死亡率分别为14.6%、35.7%、41.6%。多因素Cox分析显示年龄(≥80岁vs<50岁,P<0.001)、性别(男vs女,P<0.001)、肿瘤部位(下段vs中段,P=0.013)、病理分期(腺癌vs鳞癌,P=0.012),分化程度(差分化vs分化良好,P<0.001),TNM分期(Ⅳ vs Ⅰ,P<0.001),肿瘤大小(>50 mm vs 0~20 mm,P<0.001),化疗(是vs否,P<0.001),淋巴结比率(>0.25 vs 0,P<0.001)是食管癌患者术后远期生存的独立危险因素,并基于该模型构建了列线图,用于预测患者术后1年、3年、5年的存活概率。在训练队列中,用于预测总生存率(OS)和癌症特异性生存率(CSS)的列线图C指数分别为0.726(95%CI: 0.714-0.738)和0.735(95%CI: 0.727-0.743)。列线图在内部验证队列和外部验证队列中得到了很好的验证,内部验证队列中预测OS和CSS的C指数分别为0.752(95% CI: 0.738-0.765)和0.804(95% CI: 0.790-0.817),外部验证队列中预测OS和CSS的C指数分别为0.749(95%CI: 0.736-0.767)和0.788(95%CI: 0.751-0.808)。根据ROC曲线下面积(AUC),在预测食管癌远期预后中,该列线图显示出比肿瘤淋巴结转移(TNM)分期系统更高的敏感性。
结论: 构建的临床预测模型有较高的预测效能,能够有助于鉴别术后高危食管癌患者,可以作为TNM分期系统的补充。
Keywords: SEER database; cancer-specific survival; esophageal carcinoma; nomogram; overall survival; prognosis.
Figures


References
-
- Guo JH, Xing GL, Fang XH, et al. Proteomic profiling of fetal esophageal epithelium, esophageal cancer, and tumor-adjacent esophageal epithelium and immunohistochemical characterization of a representative differential protein, PRX6. World J Gastroenterol. 2017;23(8):1434–42. doi: 10.3748/wjg.v23.i8.1434. [Guo JH, Xing GL, Fang XH, et al. Proteomic profiling of fetal esophageal epithelium, esophageal cancer, and tumor-adjacent esophageal epithelium and immunohistochemical characterization of a representative differential protein, PRX6[J]. World J Gastroenterol, 2017, 23(8): 1434-42.] - DOI - PMC - PubMed
-
- Vingeliene S, Chan DSM, Vieira AR, et al. An update of the WCRF/ AICR systematic literature review and meta-analysis on dietary and anthropometric factors and esophageal cancer risk. Ann Oncol. 2017;28(10):2409–19. doi: 10.1093/annonc/mdx338. [Vingeliene S, Chan DSM, Vieira AR, et al. An update of the WCRF/ AICR systematic literature review and meta-analysis on dietary and anthropometric factors and esophageal cancer risk[J]. Ann Oncol, 2017, 28(10): 2409-19.] - DOI - PMC - PubMed
-
- Yu XL, Yang J, Chen T, et al. Excessive pretreatment weight loss is a risk factor for the survival outcome of esophageal carcinoma patients undergoing radical surgery and postoperative adjuvant chemotherapy. Can J Gastroenterol Hepatol. 2018;18(2):6075207. [Yu XL, Yang J, Chen T, et al. Excessive pretreatment weight loss is a risk factor for the survival outcome of esophageal carcinoma patients undergoing radical surgery and postoperative adjuvant chemotherapy[J]. Can J Gastroenterol Hepatol, 2018, 18(2): 6075207.] - PMC - PubMed
-
- Lu QJ, Bo YC, Zhao Y, et al. Glutathione S-transferase M1 polymorphism and esophageal cancer risk: an updated metaanalysis based on 37 studies. World J Gastroenterol. 2016;22(5):1911–8. doi: 10.3748/wjg.v22.i5.1911. [Lu QJ, Bo YC, Zhao Y, et al. Glutathione S-transferase M1 polymorphism and esophageal cancer risk: an updated metaanalysis based on 37 studies[J]. World J Gastroenterol, 2016, 22(5): 1911-8.] - DOI - PMC - PubMed
-
- Cummings LC, Kou TD, Schluchter MD, et al. Outcomes after endoscopic versus surgical therapy for early esophageal cancers in an older population. Gastrointest Endosc. 2016;84(2):232–40.e1. doi: 10.1016/j.gie.2016.01.019. [Cummings LC, Kou TD, Schluchter MD, et al. Outcomes after endoscopic versus surgical therapy for early esophageal cancers in an older population[J]. Gastrointest Endosc, 2016, 84(2): 232-40.e1.] - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical