

Optimal Rhythm Control Strategy in Patients With Atrial Fibrillation
- PMID: 35790494
- PMCID: PMC9257152
- DOI: 10.4070/kcj.2022.0078
Optimal Rhythm Control Strategy in Patients With Atrial Fibrillation
Abstract
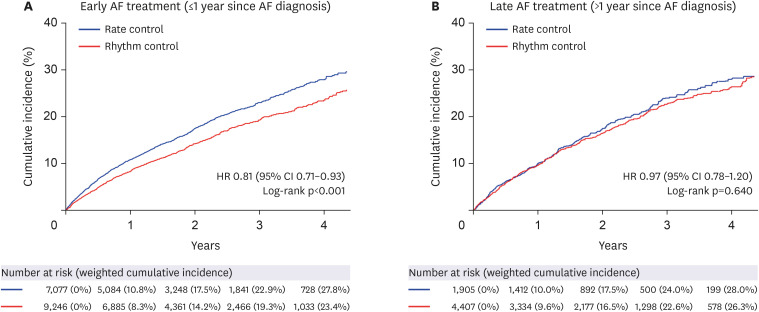
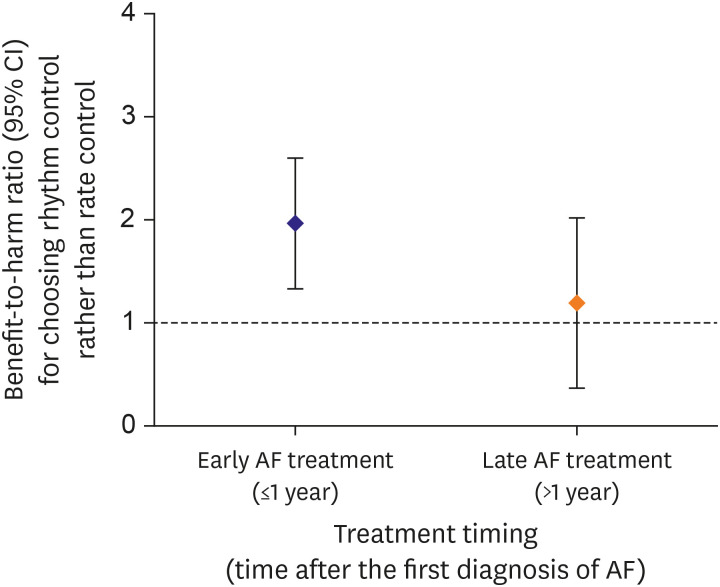
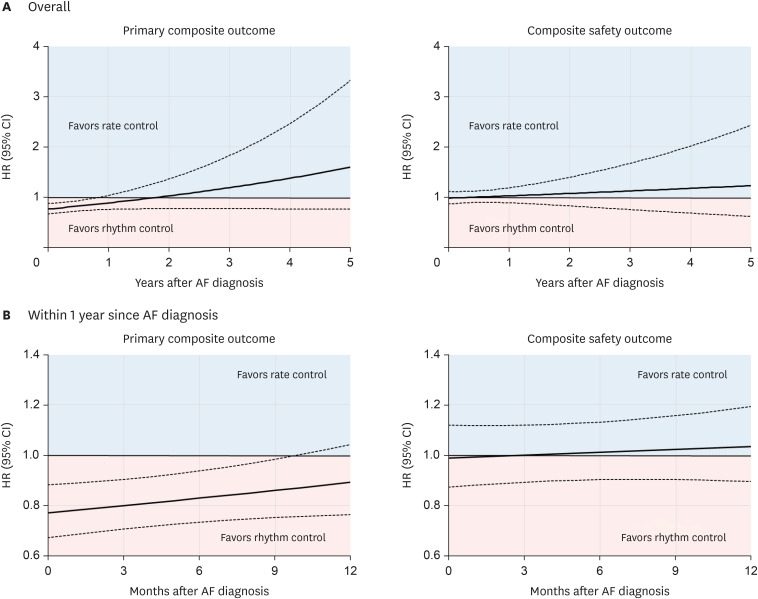
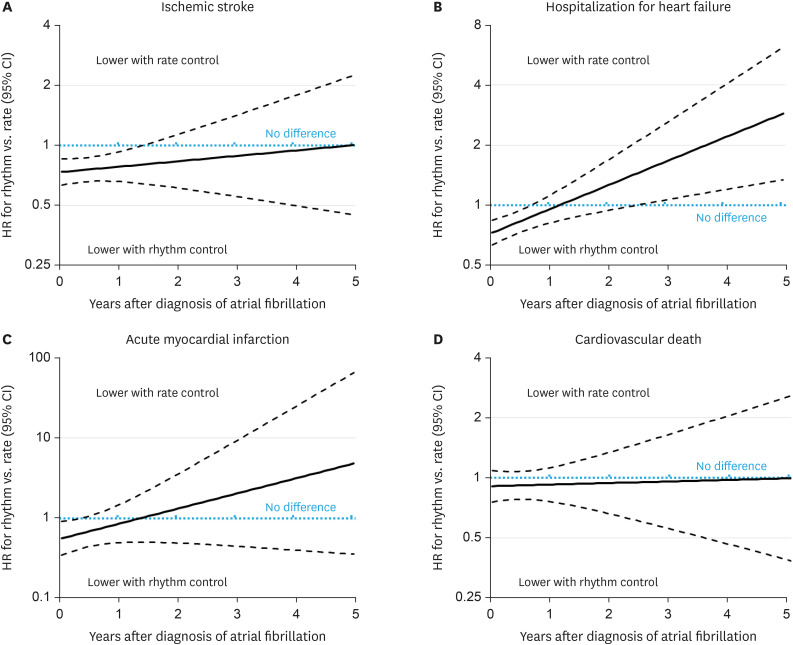
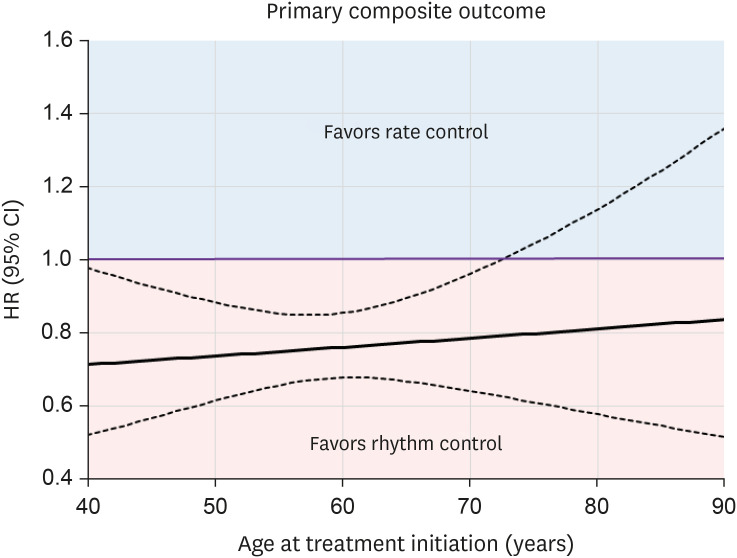
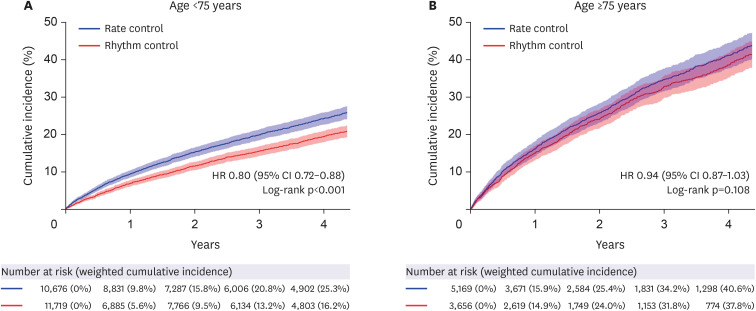
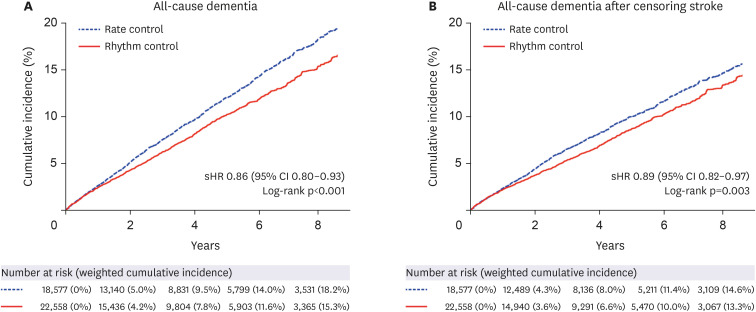
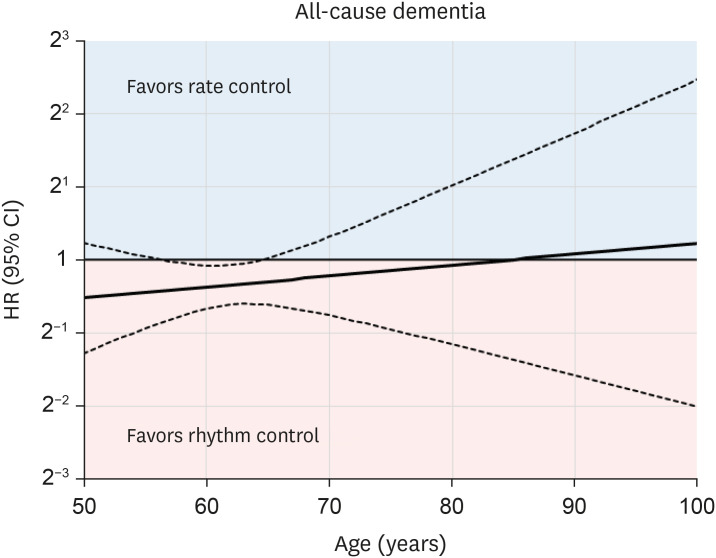
For almost 20 years, data regarding the effect of rhythm control therapy for atrial fibrillation (AF) on cardiovascular prognosis in comparison with rate control therapy has not been conclusive. The safety of rhythm control and anticoagulation therapy has generally improved. Recently, it was revealed that a rhythm-control strategy reduced the risk of adverse cardiovascular events than usual rate control in patients with recent AF (diagnosed within 1 year). Within 1 year after the AF diagnosis, early initiation of rhythm control led to more favorable cardiovascular outcomes than rate control. Early rhythm control reduced the risks of stroke and heart failure-related admission than rate control. Moreover, rhythm control was associated with lower dementia risk than rate control. Finally, early rhythm control treatment was also effective in patients with asymptomatic AF but less effective in older adults. Therefore, in patients with AF, rhythm control should be considered at earlier stages, regardless of symptom.
Keywords: Atrial fibrillation; Cardiovascular outcome; Cognitive outcome; Early treatment; Rhythm control.
Copyright © 2022. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Timmis A, Townsend N, Gale CP, et al. European Society of Cardiology: cardiovascular disease statistics 2019. Eur Heart J. 2020;41:12–85. - PubMed
-
- Kim D, Yang PS, Jang E, et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. 2018;202:20–26. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
