

Long-term quality of life after ETV or ETV with consecutive VP shunt placement in hydrocephalic pediatric patients
- PMID: 35790573
- PMCID: PMC9522746
- DOI: 10.1007/s00381-022-05590-9
Long-term quality of life after ETV or ETV with consecutive VP shunt placement in hydrocephalic pediatric patients
Erratum in
-
Correction to: Long‑term quality of life after ETV or ETV with consecutive VP shunt placement in hydrocephalic pediatric patients.Childs Nerv Syst. 2022 Oct;38(10):1895. doi: 10.1007/s00381-022-05657-7. Childs Nerv Syst. 2022. PMID: 36068357 Free PMC article. No abstract available.
Abstract
Purpose: Endoscopic third ventriculostomy (ETV) and ventriculoperitoneal shunting are well-established treatments of obstructive hydrocephalus (HCP) in adult and pediatric patients. However, there is a lack of data with regard to the quality of life (QoL) of these patients during long-term follow-up METHODS: Inclusion criteria were pediatric patients with endoscopic treatment of hydrocephalus at the University Medicine Greifswald between 1993 and 2016. Patients older than 14 years at present were assessed with the Short Form-12 (SF-12) questionnaire. Patients younger than 14 years of age were assessed with the KINDL-R questionnaire that was completed by their parents. Patients' values were compared with the scores of a corresponding age-matched group of the healthy population and with patients who received later shunt treatment. Information about comorbidities, current symptoms, and educational level were gained by an additional part. Comparative analysis between patients with ETV success and failure (defined as shunt implantation after ETV) was performed.
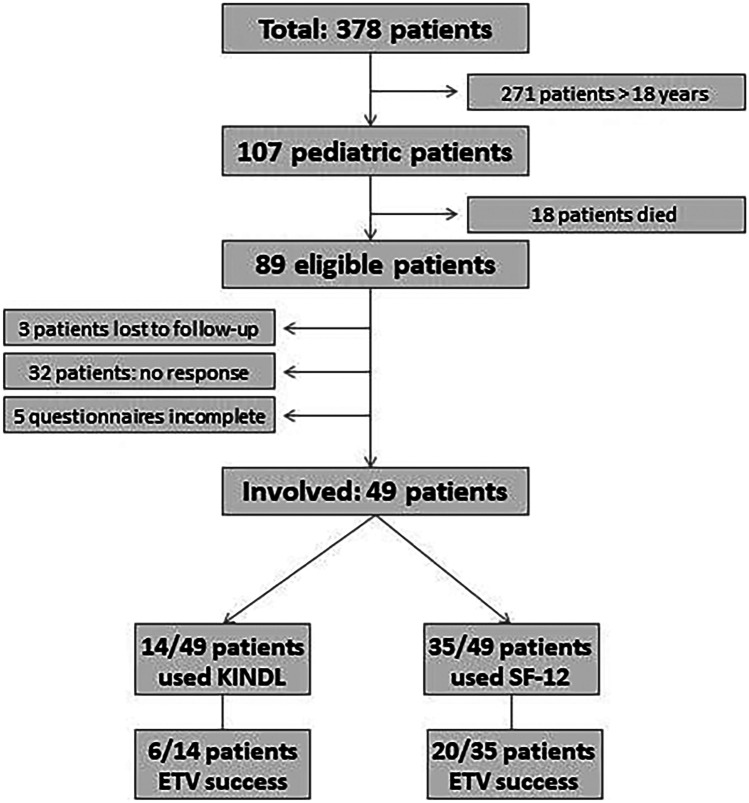
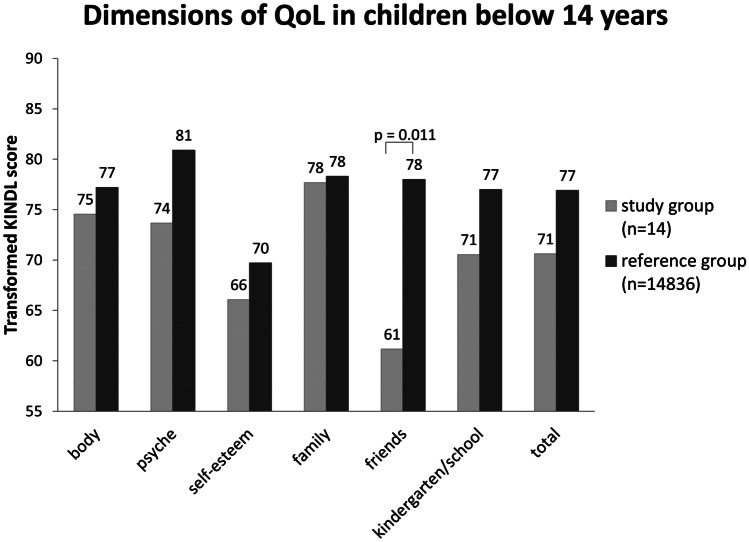
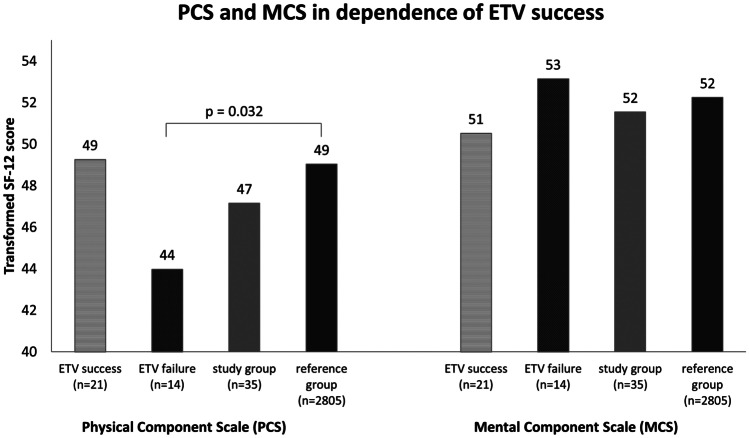
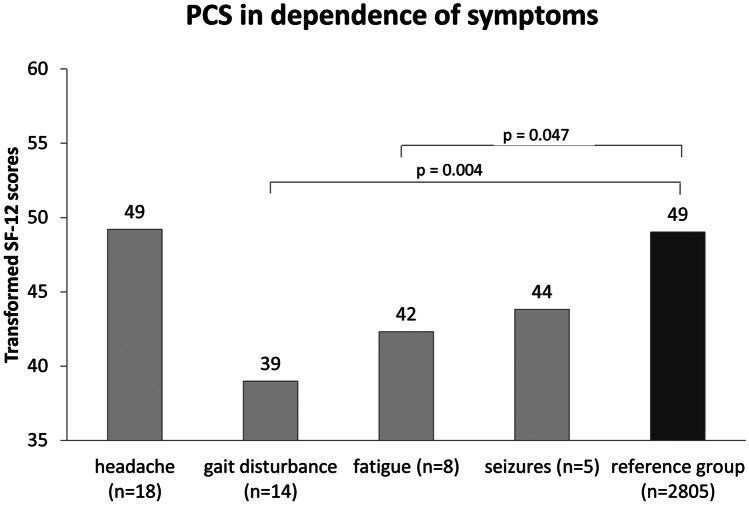
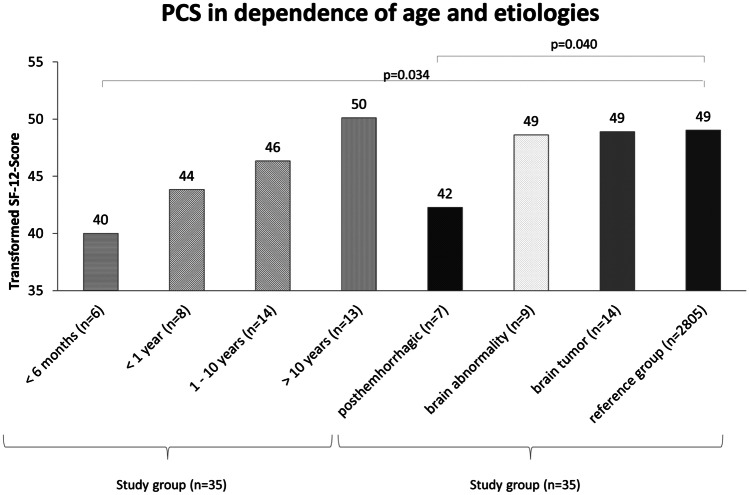
Results: A total of 107 patients (53 m, 54f) were included. Fifty-seven/107 patients (53.3%) were considered as ETV success. Mean age at ETV was 6.9 ± 5.9 years. Fifty-four statements of 89 patients that are still alive were gained (response rate 63%). Of these, 49 questionnaires were complete and evaluable (23 m, 26f; mean age 19.8 ± 10.0 years with an average follow-up period of 13.7 ± 7.2 years). Twenty-six/49 patients (53.1%) are considered ETV success. No statistically significant differences could be obtained between patients with ETV success and ETV failure. Patients older 14 years show QoL within normal range, patients younger than 14 years show significantly lower result regarding their environment of peers and social contacts. Patients younger than 6 months at the time of ETV and patients with posthemorrhagic HCP show significantly lower physical QoL. Gait disturbance, fatigue, and seizures are associated with a lower QoL, and educational level is lower than in the normal population.
Conclusions: Patients who underwent ETV in childhood do not have a lower health-related QoL in general. Subsequent insertions of ventriculoperitoneal (vp) shunts do not lower QoL. Certain subgroups of the patients show lower results compared to the healthy population.
Keywords: Endoscopic third ventriculostomy; Hydrocephalus; Pediatric; Quality of life.
© 2022. The Author(s).
Conflict of interest statement
Henry W. S. Schroeder is a consultant for Karl Storz SA & Co. KG, Tuttlingen, Germany. All other authors declare that they have no conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
