

Pharmacological treatment strategies for antipsychotic-induced hyperprolactinemia: a systematic review and network meta-analysis
- PMID: 35790713
- PMCID: PMC9256633
- DOI: 10.1038/s41398-022-02027-4
Pharmacological treatment strategies for antipsychotic-induced hyperprolactinemia: a systematic review and network meta-analysis
Abstract
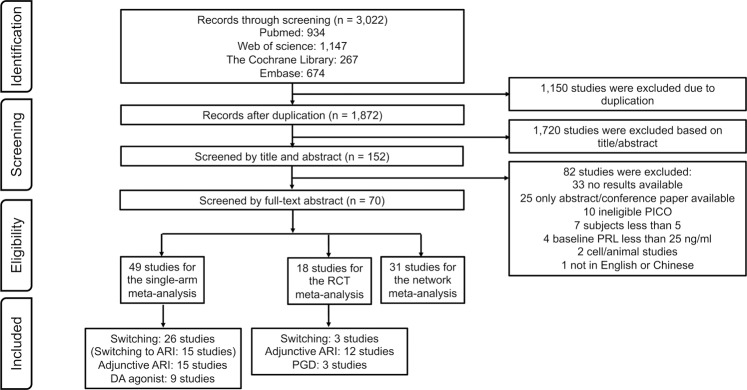
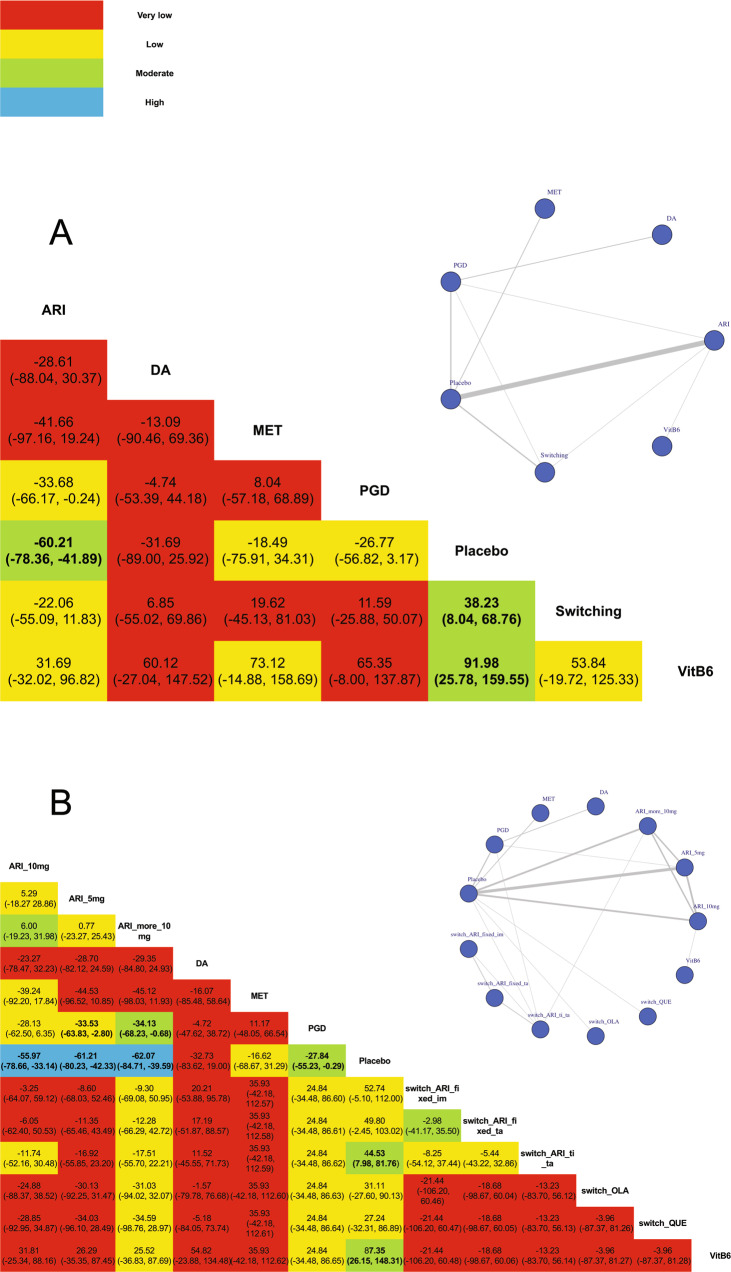
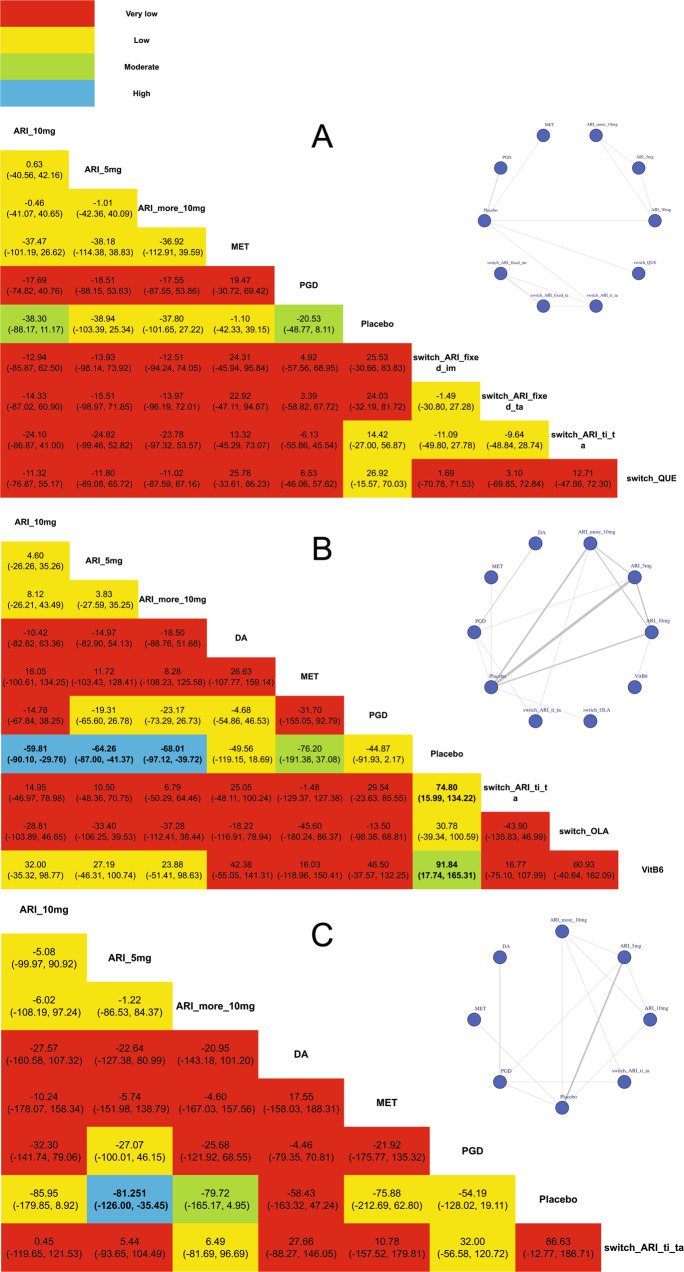
Antipsychotic-induced hyperprolactinemia (AP-induced HPRL) occurs overall in up to 70% of patients with schizophrenia, which is associated with hypogonadism and sexual dysfunction. We summarized the latest evidence for the benefits of prolactin-lowering drugs. We performed network meta-analyses to summarize the evidence and applied Grading of Recommendations Assessment, Development, and Evaluation frameworks (GRADE) to rate the certainty of evidence, categorize interventions, and present the findings. The search identified 3,022 citations, 31 studies of which with 1999 participants were included in network meta-analysis. All options were not significantly better than placebo among patients with prolactin (PRL) less than 50 ng/ml. However, adjunctive aripiprazole (ARI) (5 mg: MD = -64.26, 95% CI = -87.00 to -41.37; 10 mg: MD = -59.81, 95% CI = -90.10 to -29.76; more than 10 mg: MD = -68.01, 95% CI = -97.12 to -39.72), switching to ARI in titration (MD = -74.80, 95% CI = -134.22 to -15.99) and adjunctive vitamin B6 (MD = -91.84, 95% CI = -165.31 to -17.74) were associated with significant decrease in AP-induced PRL among patients with PRL more than 50 ng/ml with moderated (adjunctive vitamin B6) to high (adjunctive ARI) certainty of evidence. Pharmacological treatment strategies for AP-induced HPRL depends on initial PRL level. No effective strategy was found for patients with AP-induced HPRL less than 50 ng/ml, while adjunctive ARI, switching to ARI in titration and adjunctive high-dose vitamin B6 showed better PRL decrease effect on AP-induced HPRL more than 50 ng/ml.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
