

The future of intensive care: delirium should no longer be an issue
- PMID: 35790979
- PMCID: PMC9254432
- DOI: 10.1186/s13054-022-04077-y
The future of intensive care: delirium should no longer be an issue
Erratum in
-
Correction to: The future of intensive care: delirium should no longer be an issue.Crit Care. 2022 Sep 21;26(1):285. doi: 10.1186/s13054-022-04128-4. Crit Care. 2022. PMID: 36131315 Free PMC article. No abstract available.
Abstract
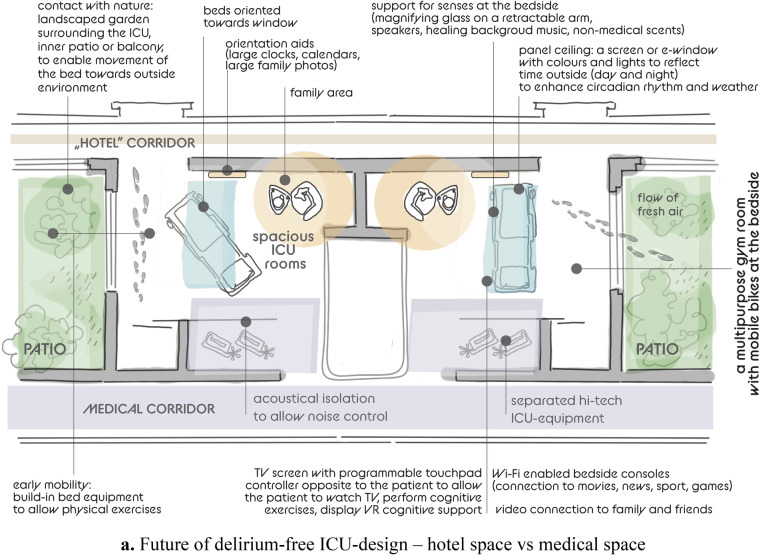
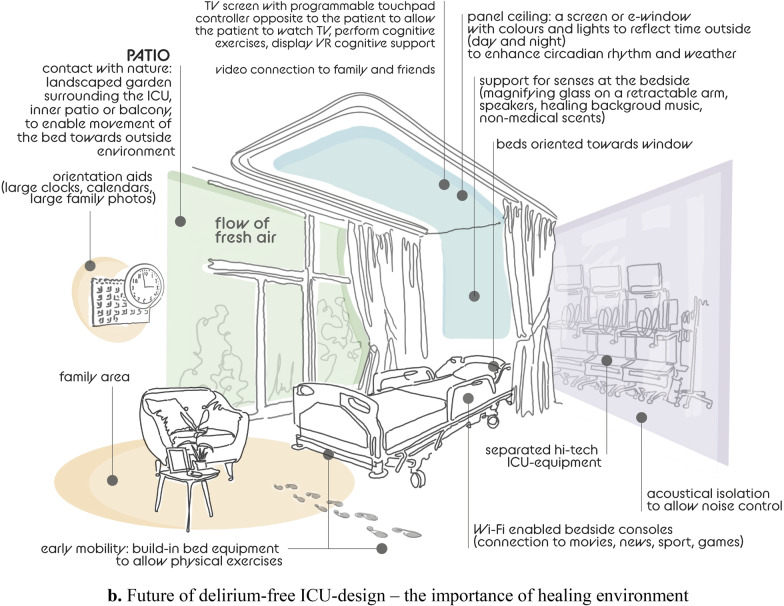
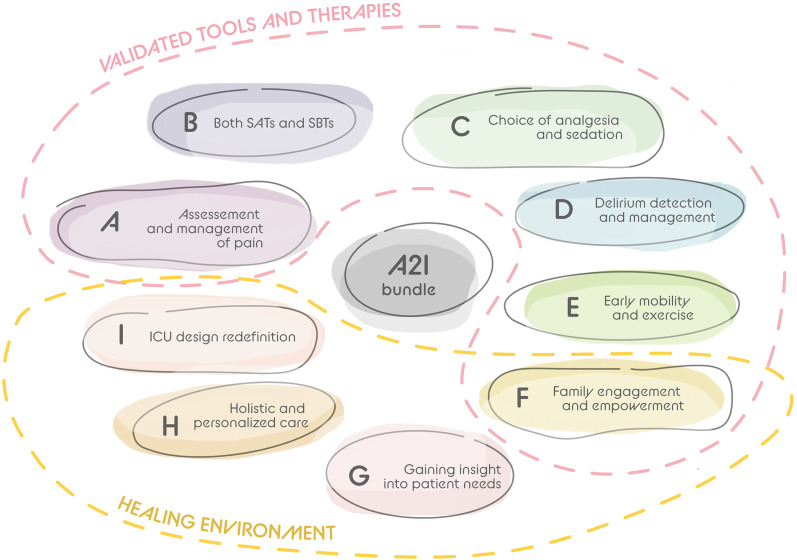
In the ideal intensive care unit (ICU) of the future, all patients are free from delirium, a syndrome of brain dysfunction frequently observed in critical illness and associated with worse ICU-related outcomes and long-term cognitive impairment. Although screening for delirium requires limited time and effort, this devastating disorder remains underestimated during routine ICU care. The COVID-19 pandemic brought a catastrophic reduction in delirium monitoring, prevention, and patient care due to organizational issues, lack of personnel, increased use of benzodiazepines and restricted family visitation. These limitations led to increases in delirium incidence, a situation that should never be repeated. Good sedation practices should be complemented by novel ICU design and connectivity, which will facilitate non-pharmacological sedation, anxiolysis and comfort that can be supplemented by balanced pharmacological interventions when necessary. Improvements in the ICU sound, light control, floor planning, and room arrangement can facilitate a healing environment that minimizes stressors and aids delirium prevention and management. The fundamental prerequisite to realize the delirium-free ICU, is an awake non-sedated, pain-free comfortable patient whose management follows the A to F (A-F) bundle. Moreover, the bundle should be expanded with three additional letters, incorporating humanitarian care: gaining (G) insight into patient needs, delivering holistic care with a 'home-like' (H) environment, and redefining ICU architectural design (I). Above all, the delirium-free world relies upon people, with personal challenges for critical care teams to optimize design, environmental factors, management, time spent with the patient and family and to humanize ICU care.
Keywords: Architecture; ICU design; Intensive care unit; Neuroesthetics; Outcome; PICS; PICS-F.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures
Comment in
-
Future without delirium: not quite there yet but we can start by prescribing touch.Crit Care. 2022 Oct 27;26(1):332. doi: 10.1186/s13054-022-04147-1. Crit Care. 2022. PMID: 36303233 Free PMC article. No abstract available.
-
Negative pressure ventilation protects the brain.Crit Care. 2022 Oct 31;26(1):334. doi: 10.1186/s13054-022-04150-6. Crit Care. 2022. PMID: 36316698 Free PMC article. No abstract available.
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. American Psychiatric Association; 2013.
-
- Pun BT, Badenes R, Heras La Calle G, et al. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): a multicentre cohort study [published correction appears in Lancet Respir Med. 2021 Jan 27;:] Lancet Respir Med. 2021;9(3):239–250. doi: 10.1016/S2213-2600(20)30552-X. - DOI - PMC - PubMed
-
- Rood P, Huisman-de Waal G, Vermeulen H, Schoonhoven L, Pickkers P, van den Boogaard M. Effect of organisational factors on the variation in incidence of delirium in intensive care unit patients: a systematic review and meta-regression analysis. Aust Crit Care. 2018;31(3):180–187. doi: 10.1016/j.aucc.2018.02.002. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
