

Anatomical variants of the acromioclavicular joint influence its visibility in the standard MRI protocol in patients aged 18-31 years
- PMID: 35792912
- PMCID: PMC9308581
- DOI: 10.1007/s00276-022-02973-0
Anatomical variants of the acromioclavicular joint influence its visibility in the standard MRI protocol in patients aged 18-31 years
Abstract
Purpose: Visualization of a structure in orthogonal planes is essential for correct radiological assessment. The aim was to assess the utility of the standard MRI protocol for the shoulder in the assessment of the acromioclavicular joint (ACJ).
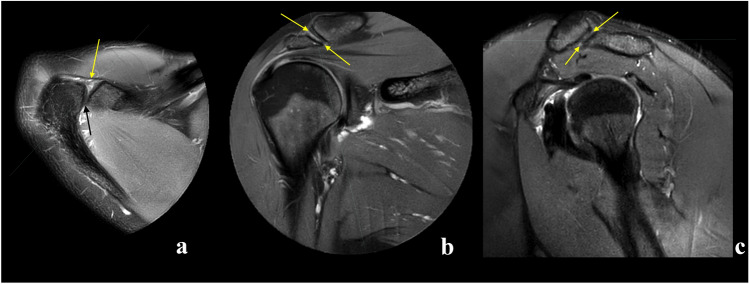
Methods: A total of 204 MRI scans of the shoulder were re-reviewed. Visibility of the ACJ in orthogonal planes was assessed, and the type of acromion and the angle between the ACJ and the glenoid cavity were assessed by two observers.
Results: Agreement in the assessment of ACJ visibility was moderate to substantial. The ACJ was visible in the three anatomical views in 48% (confidence interval [CI] 95% = [41-54%]) of the examinations, and no significant difference regarding gender or age was noticed. The mean angle between the ACJ and the glenoid cavity was 41.12 deg. CI95% = (39.72, 42.53) in the axial plane, 33.39 deg. CI95% = (31.33, 35.45) in the coronal plane and 52.49 deg. CI95% = (50.10, 54.86) in the sagittal plane. When the ACJ was visible in the sagittal and axial planes, significant differences were noticed in the remaining planes (p < .05).
Conclusion: Anatomical variations of the ACJ influence its visibility in the standard MRI protocol for examining the shoulder, making this protocol insufficient for ACJ assessment in the examined population.
Keywords: Acromioclavicular joint; Acromion; Anatomy; Magnetic resonance imaging; Shoulder pain.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








Similar articles
-
Evaluation of the Circles Measurement and the ABC Classification of Acromioclavicular Joint Injuries.Am J Sports Med. 2021 May;49(6):1619-1625. doi: 10.1177/03635465211003300. Epub 2021 Apr 15. Am J Sports Med. 2021. PMID: 33856933
-
New quantitative radiographic parameters for vertical and horizontal instability in acromioclavicular joint dislocations.Knee Surg Sports Traumatol Arthrosc. 2018 Jan;26(1):125-135. doi: 10.1007/s00167-017-4579-6. Epub 2017 May 25. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 28547587 Free PMC article.
-
Morphological Characteristics of Acromion and Acromioclavicular Joint in Patients with Shoulder Impingement Syndrome and Related Recommendations: A Three-Dimensional Analysis Based on Multiplanar Reconstruction of Computed Tomography Scans.Orthop Surg. 2021 Jun;13(4):1309-1318. doi: 10.1111/os.13001. Epub 2021 May 6. Orthop Surg. 2021. PMID: 33955185 Free PMC article.
-
Acromioclavicular Joint: What to Look for.Magn Reson Imaging Clin N Am. 2020 May;28(2):269-283. doi: 10.1016/j.mric.2019.12.009. Epub 2020 Feb 19. Magn Reson Imaging Clin N Am. 2020. PMID: 32241663 Review.
-
The relationship of the acromion to the distal clavicle in normal and symptomatic degenerated acromioclavicular joints.Arch Orthop Trauma Surg. 2020 Apr;140(4):465-472. doi: 10.1007/s00402-019-03258-9. Epub 2019 Aug 19. Arch Orthop Trauma Surg. 2020. PMID: 31428850 Review.
Cited by
-
Unraveling Anatomical Variations of the Acromioclavicular Joint: A Comprehensive Inquiry Into Their Impact on Instability.Cureus. 2024 Dec 6;16(12):e75197. doi: 10.7759/cureus.75197. eCollection 2024 Dec. Cureus. 2024. PMID: 39759629 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
