

Effect of manipulation technique using ultrasound-guided cervical nerve root block on range of motion at the shoulder joint in frozen shoulder: a retrospective study
- PMID: 35792941
- PMCID: PMC9259775
- DOI: 10.1186/s40634-022-00500-z
Effect of manipulation technique using ultrasound-guided cervical nerve root block on range of motion at the shoulder joint in frozen shoulder: a retrospective study
Abstract
Purpose: The aim of this study was to evaluate the range of motion (ROM) at the shoulder joint before and after silent manipulation.
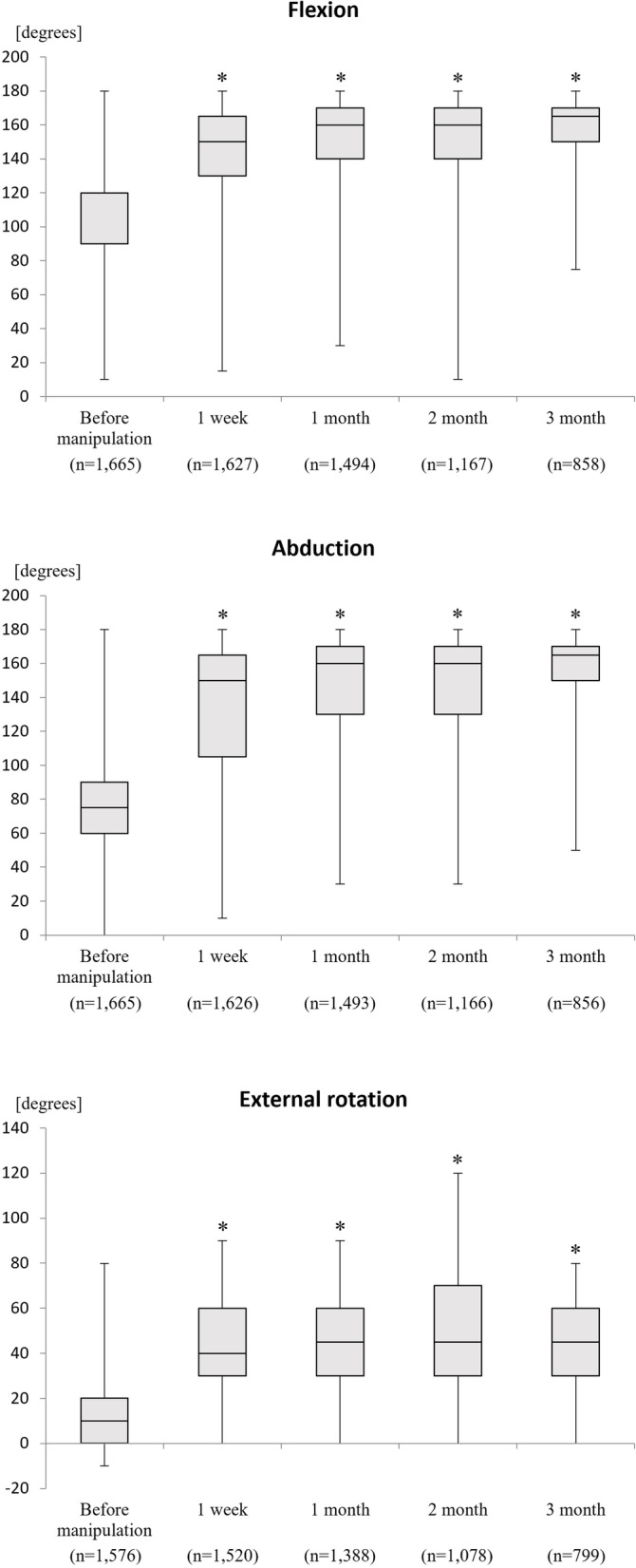
Methods: This retrospective study included all patients who underwent silent manipulation at our institution between January 2013 and December 2017. In total, 1,665 shoulders in 1,610 patients (519 men, 1,146 women; mean age 55.4 ± 8.8 years) were treated during the study period. The mean symptom duration was 6.6 ± 7.1 months. ROM at the shoulder joint was measured in flexion, abduction, and external rotation before silent manipulation and at 1 week and 1, 2, and 3 months after the procedure.
Results: Mean ROM at the shoulder was 98.8° (95% confidence interval [CI] 97.9-99.8) before silent manipulation and 155.5° (154.1-156.8) after 3 months in flexion (p = 0.0000), 75.6° (74.5-76.8) and 152.9° (151.0-154.9), respectively, in abduction (p = 0.0000), and 12.7° (12.0-13.4) and 45.9° (44.4-47.4) in external rotation (p = 0.0000). All ROM values were significantly increased at all time points after the procedure. There were no unanticipated adverse events or serious adverse reactions.
Conclusions: This study reports on the efficacy and safety of manipulation using conduction anesthesia for shoulder contractures in a large group of patients. Silent manipulation can increase ROM at the shoulder safely and effectively.
Keywords: Adhesion; Frozen shoulder; Silent manipulation; Ultrasound-guided cervical nerve root block.
© 2022. The Author(s).
Conflict of interest statement
None
Figures






References
-
- Miyatake K, Fujisawa T, Otoshi A, Kawabata Y, Kusaba Y, Tsujiku S, Inaba Y. Silent manipulation for adhesive capsulitis. Curr Phys Med Rehabil Rep. 2021;9:230–236. doi: 10.1007/s40141-021-00332-5. - DOI
LinkOut - more resources
Full Text Sources
