

Brain age estimation reveals older adults' accelerated senescence after traumatic brain injury
- PMID: 35792961
- PMCID: PMC9768106
- DOI: 10.1007/s11357-022-00597-1
Brain age estimation reveals older adults' accelerated senescence after traumatic brain injury
Abstract
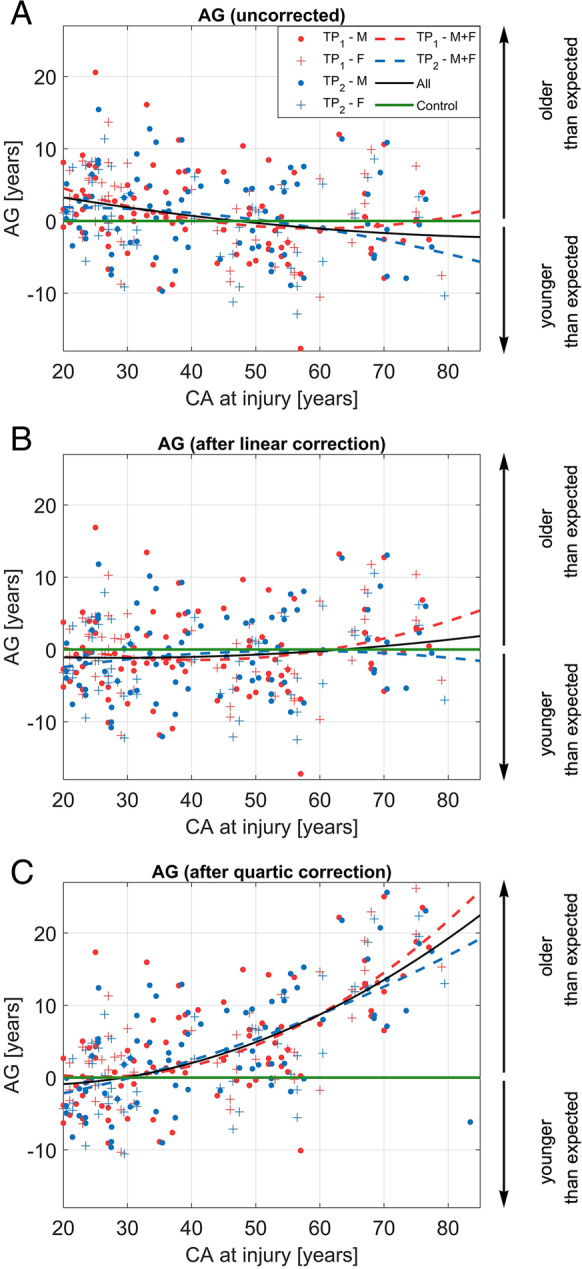
Adults aged 60 and over are most vulnerable to mild traumatic brain injury (mTBI). Nevertheless, the extent to which chronological age (CA) at injury affects TBI-related brain aging is unknown. This study applies Gaussian process regression to T1-weighted magnetic resonance images (MRIs) acquired within [Formula: see text]7 days and again [Formula: see text]6 months after a single mTBI sustained by 133 participants aged 20-83 (CA [Formula: see text] = 42.6 ± 17 years; 51 females). Brain BAs are estimated, modeled, and compared as a function of sex and CA at injury using a statistical model selection procedure. On average, the brains of older adults age by 15.3 ± 6.9 years after mTBI, whereas those of younger adults age only by 1.8 ± 5.6 years, a significant difference (Welch's t32 = - 9.17, p ≃ 9.47 × 10-11). For an adult aged [Formula: see text]30 to [Formula: see text]60, the expected amount of TBI-related brain aging is [Formula: see text]3 years greater than in an individual younger by a decade. For an individual over [Formula: see text]60, the respective amount is [Formula: see text]7 years. Despite no significant sex differences in brain aging (Welch's t108 = 0.78, p > 0.78), the statistical test is underpowered. BAs estimated at acute baseline versus chronic follow-up do not differ significantly (t264 = 0.41, p > 0.66, power = 80%), suggesting negligible TBI-related brain aging during the chronic stage of TBI despite accelerated aging during the acute stage. Our results indicate that a single mTBI sustained after age [Formula: see text]60 involves approximately [Formula: see text]10 years of premature and lasting brain aging, which is MRI detectable as early as [Formula: see text]7 days post-injury.
Keywords: Biological age; Chronological age; Machine learning; Magnetic resonance imaging; Neurodegeneration.
© 2022. The Author(s), under exclusive licence to American Aging Association.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
