

Faecal incontinence is associated with an impaired rectosigmoid brake and improved by sacral neuromodulation
- PMID: 35793162
- PMCID: PMC10084032
- DOI: 10.1111/codi.16249
Faecal incontinence is associated with an impaired rectosigmoid brake and improved by sacral neuromodulation
Abstract
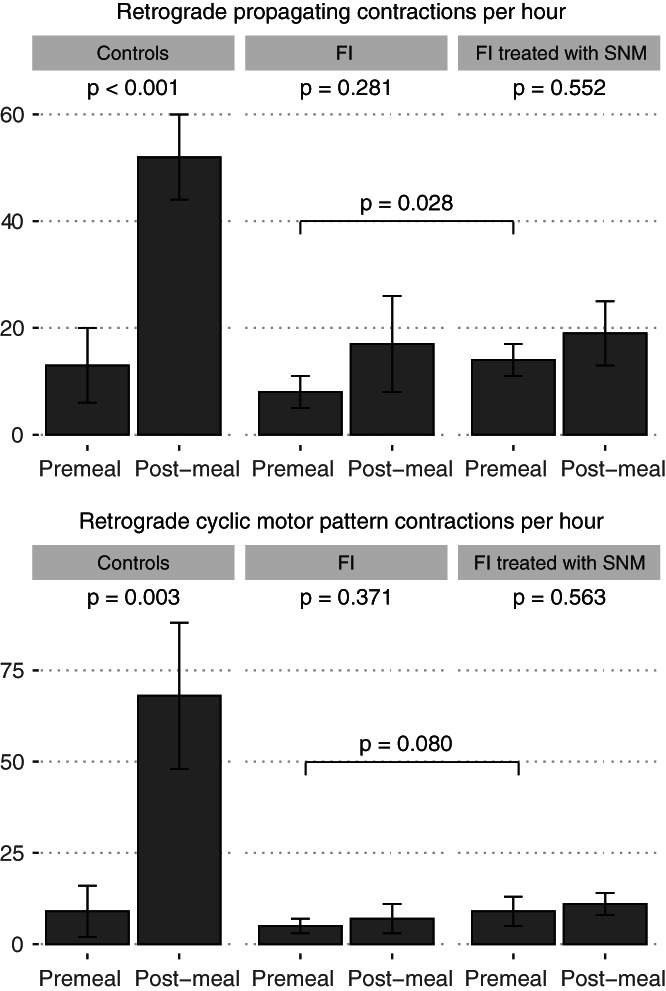
Background: The rectosigmoid brake, characterised by retrograde cyclic motor patterns on high-resolution colonic manometry, has been postulated as a contributor to the maintenance of bowel continence. Sacral neuromodulation (SNM) is an effective therapy for faecal incontinence, but its mechanism of action is unclear. This study aims to investigate the colonic motility patterns in the distal colon of patients with faecal incontinence, and how these are modulated by SNM.
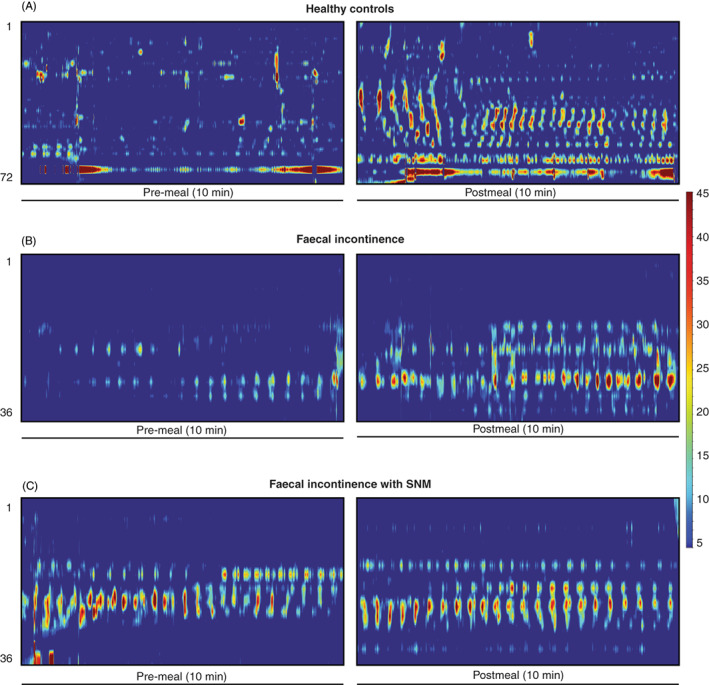
Methods: A high-resolution fibreoptic colonic manometry catheter, containing 36 sensors spaced at 1-cm intervals, was positioned in patients with faecal incontinence undergoing stage 1 SNM. One hour of pre- and post meal recordings were obtained followed by pre- and post meal recordings with suprasensory SNM. A 700-kcal meal was given. Data were analysed to identify propagating contractions.
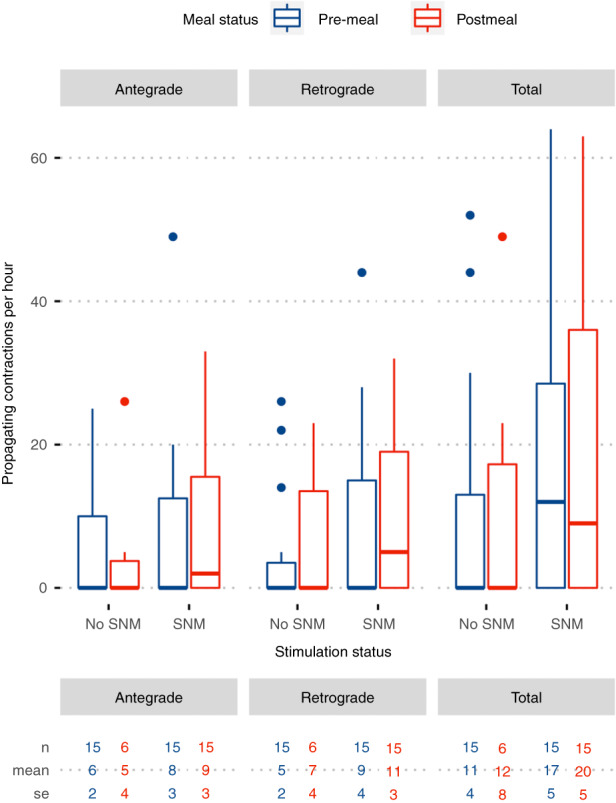
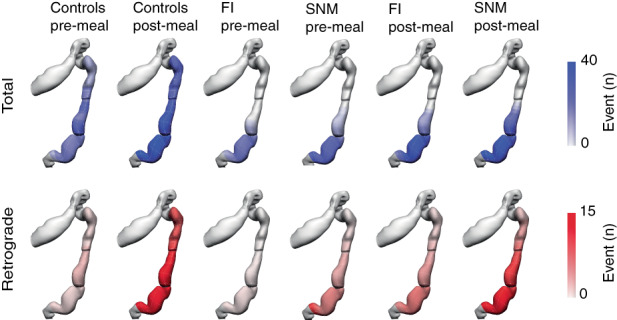
Results: Fifteen patients with faecal incontinence were analysed. Patients had an abnormal meal response (fewer retrograde propagating contractions compared to controls; p = 0.027) and failed to show a post meal increase in propagating contractions (mean 17 ± 6/h premeal vs. 22 ± 9/h post meal, p = 0.438). Compared to baseline, SNM significantly increased the number of retrograde propagating contractions in the distal colon (8 ± 3/h premeal vs. 14 ± 3/h premeal with SNM, p = 0.028). Consuming a meal did not further increase the number of propagating contractions beyond the baseline upregulating effect of SNM.
Conclusion: The rectosigmoid brake was suppressed in this cohort of patients with faecal incontinence. SNM may exert a therapeutic effect by modulating this rectosigmoid brake.
Keywords: faecal incontinence; implant; rectosigmoid brake; sacral nerve stimulation; sacral neuromodulation.
© 2022 The Authors. Colorectal Disease published by John Wiley & Sons Ltd on behalf of Association of Coloproctology of Great Britain and Ireland.
Conflict of interest statement
GOG is a shareholder and Director of Alimetry and The Insides Company and holds intellectual property in the field of gastrointestinal electrophysiology and therapeutics. IB is a shareholder in the Insides Company. NP and PD hold intellectual property in the field of gastric electrophysiology and is a shareholder in FlexiMap Ltd. No commercial financial support was received for this study. All remaining authors (AL, CV, NP, SS, PD) have no conflicts of interest to declare.
Figures
Similar articles
-
The effect of sacral nerve stimulation on distal colonic motility in patients with faecal incontinence.Br J Surg. 2013 Jun;100(7):959-68. doi: 10.1002/bjs.9114. Epub 2013 Mar 27. Br J Surg. 2013. PMID: 23536312 Clinical Trial.
-
Sacral neuromodulation; does it affect colonic transit time in patients with faecal incontinence?Colorectal Dis. 2006 May;8(4):318-22. doi: 10.1111/j.1463-1318.2005.00930.x. Colorectal Dis. 2006. PMID: 16630237 Clinical Trial.
-
High-resolution anatomic correlation of cyclic motor patterns in the human colon: Evidence of a rectosigmoid brake.Am J Physiol Gastrointest Liver Physiol. 2017 May 1;312(5):G508-G515. doi: 10.1152/ajpgi.00021.2017. Epub 2017 Mar 23. Am J Physiol Gastrointest Liver Physiol. 2017. PMID: 28336544 Free PMC article.
-
Sacral neuromodulation in patients with congenital faecal incontinence. Special issues and review of the literature.Tech Coloproctol. 2018 Feb;22(2):89-95. doi: 10.1007/s10151-017-1742-5. Epub 2018 Jan 16. Tech Coloproctol. 2018. PMID: 29340832 Review.
-
The role of sacral neuromodulation in double incontinence.Colorectal Dis. 2011 Mar;13 Suppl 2:15-8. doi: 10.1111/j.1463-1318.2010.02520.x. Colorectal Dis. 2011. PMID: 21284797 Review.
Cited by
-
Validation of body surface colonic mapping (BSCM) against high resolution colonic manometry for evaluation of colonic motility.Sci Rep. 2024 Feb 28;14(1):4842. doi: 10.1038/s41598-024-54429-7. Sci Rep. 2024. PMID: 38418514 Free PMC article.
-
The role of colonic motility in low anterior resection syndrome.Front Oncol. 2022 Sep 16;12:975386. doi: 10.3389/fonc.2022.975386. eCollection 2022. Front Oncol. 2022. PMID: 36185226 Free PMC article. Review.
-
Sacral Neuromodulation in Patients With Low Anterior Resection Syndrome: The SANLARS Randomized Clinical Trial.Dis Colon Rectum. 2024 Mar 1;67(3):435-447. doi: 10.1097/DCR.0000000000003143. Epub 2023 Dec 11. Dis Colon Rectum. 2024. PMID: 38084933 Free PMC article. Clinical Trial.
-
Management of Low Anterior Resection Syndrome (LARS) Following Resection for Rectal Cancer.Cancers (Basel). 2023 Jan 27;15(3):778. doi: 10.3390/cancers15030778. Cancers (Basel). 2023. PMID: 36765736 Free PMC article. Review.
-
High output stoma after surgery for rectal cancer - a risk factor for low anterior resection syndrome?BMC Gastroenterol. 2025 Jan 23;25(1):32. doi: 10.1186/s12876-025-03614-7. BMC Gastroenterol. 2025. PMID: 39849372 Free PMC article.
References
-
- Sharma A, Yuan L, Marshall RJ, Merrie AEH, Bissett IP. Systematic review of the prevalence of faecal incontinence. Br J Surg. 2016;103:1589–97. - PubMed
-
- Xu X, Menees SB, Zochowski MK, Fenner DE. Economic cost of fecal incontinence. Dis Colon Rectum. 2012;55:586–98. - PubMed
-
- Nehra V, Bruce BK, Rath‐Harvey DM, Pemberton JH, Camilleri M. Psychological disorders in patients with evacuation disorders and constipation in a tertiary practice. Am J Gastroenterol. 2000;95:1755–8. - PubMed
-
- Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon Rectum. 1993;36:77–97. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
