

Racial bias and reproducibility in pulse oximetry among medical and surgical inpatients in general care in the Veterans Health Administration 2013-19: multicenter, retrospective cohort study
- PMID: 35793817
- PMCID: PMC9254870
- DOI: 10.1136/bmj-2021-069775
Racial bias and reproducibility in pulse oximetry among medical and surgical inpatients in general care in the Veterans Health Administration 2013-19: multicenter, retrospective cohort study
Abstract
Objectives: To evaluate measurement discrepancies by race between pulse oximetry and arterial oxygen saturation (as measured in arterial blood gas) among inpatients not in intensive care.
Design: Multicenter, retrospective cohort study using electronic medical records from general care medical and surgical inpatients.
Setting: Veteran Health Administration, a national and racially diverse integrated health system in the United States, from 2013 to 2019.
Participants: Adult inpatients in general care (medical and surgical), in Veteran Health Administration medical centers.
Main outcomes measures: Occult hypoxemia (defined as arterial blood oxygen saturation (SaO2) of <88% despite a pulse oximetry (SpO2) reading of ≥92%), and whether rates of occult hypoxemia varied by race and ethnic origin.
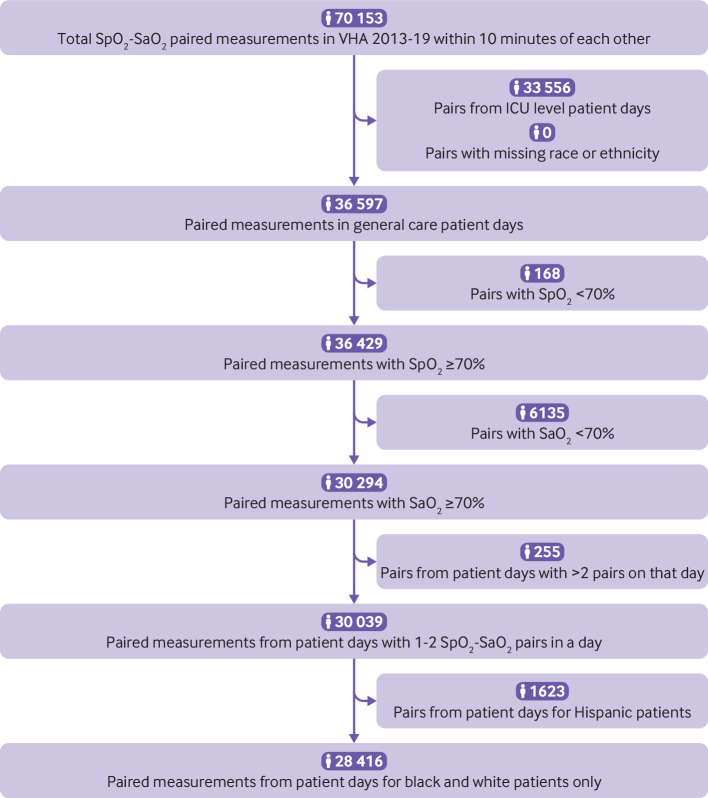
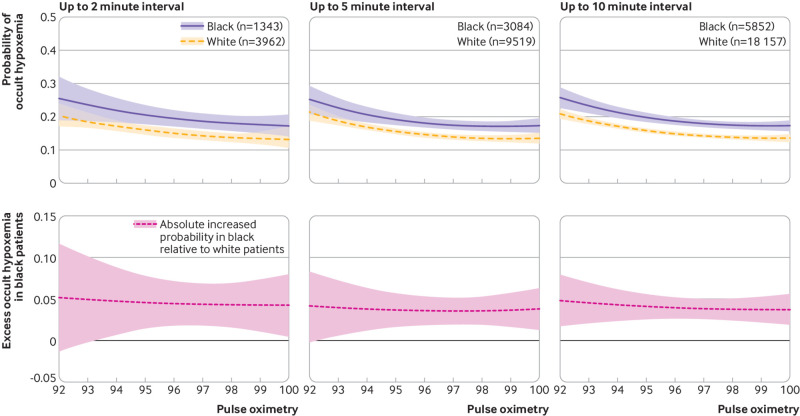
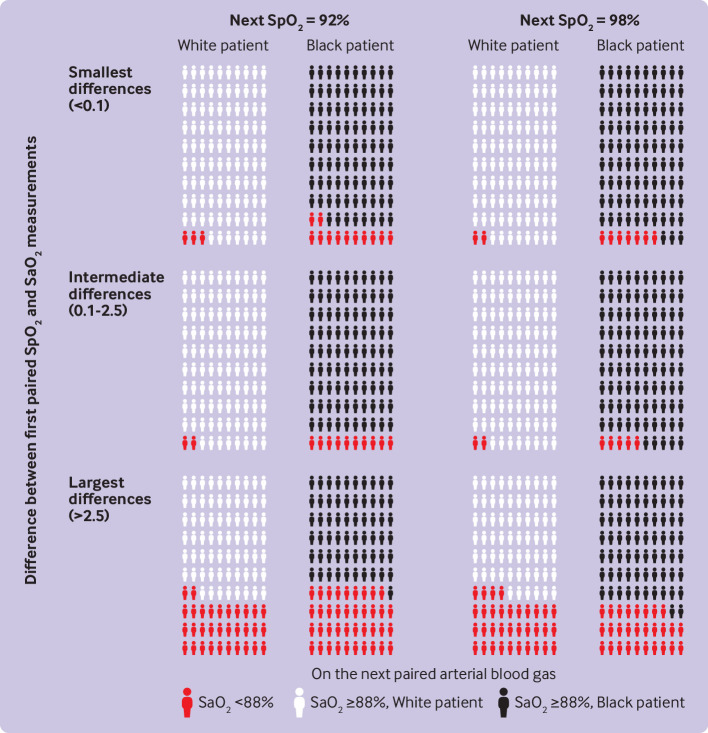
Results: A total of 30 039 pairs of SpO2-SaO2 readings made within 10 minutes of each other were identified during the study. These pairs were predominantly among non-Hispanic white (21 918 (73.0%)) patients; non-Hispanic black patients and Hispanic or Latino patients accounted for 6498 (21.6%) and 1623 (5.4%) pairs in the sample, respectively. Among SpO2 values greater or equal to 92%, unadjusted probabilities of occult hypoxemia were 15.6% (95% confidence interval 15.0% to 16.1%) in white patients, 19.6% (18.6% to 20.6%) in black patients (P<0.001 v white patients, with similar P values in adjusted models), and 16.2% (14.4% to 18.1%) in Hispanic or Latino patients (P=0.53 v white patients, P<0.05 in adjusted models). This result was consistent in SpO2-SaO2 pairs restricted to occur within 5 minutes and 2 minutes. In white patients, an initial SpO2-SaO2 pair with little difference in saturation was associated with a 2.7% (95% confidence interval -0.1% to 5.5%) probability of SaO2 <88% on a later paired SpO2-SaO2 reading showing an SpO2 of 92%, but black patients had a higher probability (12.9% (-3.3% to 29.0%)).
Conclusions: In general care inpatient settings across the Veterans Health Administration where paired readings of arterial blood gas (SaO2) and pulse oximetry (SpO2) were obtained, black patients had higher odds than white patients of having occult hypoxemia noted on arterial blood gas but not detected by pulse oximetry. This difference could limit access to supplemental oxygen and other more intensive support and treatments for black patients.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the National Institutes of Health, Veterans Affairs Administration, Agency for Healthcare Research and Quality, National Health Lung and Blood Institute of the National Institutes of Health, and National Clinician Scholars Program for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical