

C reactive protein utilisation, a biomarker for early COVID-19 treatment, improves lenzilumab efficacy: results from the randomised phase 3 'LIVE-AIR' trial
- PMID: 35793833
- PMCID: PMC10314034
- DOI: 10.1136/thoraxjnl-2022-218744
C reactive protein utilisation, a biomarker for early COVID-19 treatment, improves lenzilumab efficacy: results from the randomised phase 3 'LIVE-AIR' trial
Abstract
Objective: COVID-19 severity is correlated with granulocyte macrophage colony-stimulating factor (GM-CSF) and C reactive protein (CRP) levels. In the phase three LIVE-AIR trial, lenzilumab an anti-GM-CSF monoclonal antibody, improved the likelihood of survival without ventilation (SWOV) in COVID-19, with the greatest effect in participants having baseline CRP below a median of 79 mg/L. Herein, the utility of baseline CRP to guide lenzilumab treatment was assessed.
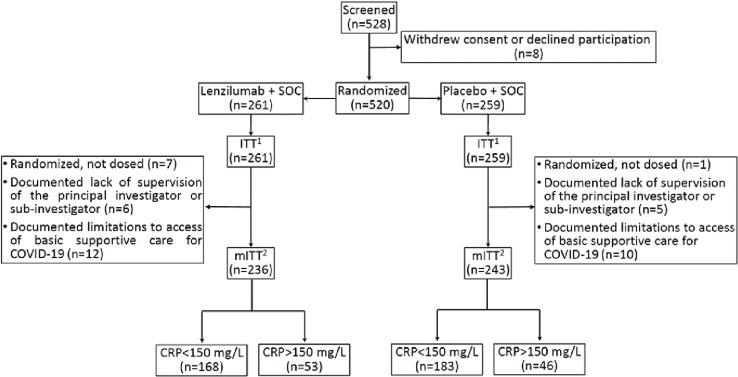
Design: A subanalysis of the randomised, blinded, controlled, LIVE-AIR trial in which lenzilumab or placebo was administered on day 0 and participants were followed through Day 28.
Participants: Hospitalised COVID-19 participants (N=520) with SpO2 ≤94% on room air or requiring supplemental oxygen but not invasive mechanical ventilation.
Interventions: Lenzilumab (1800 mg; three divided doses, q8h, within 24 hours) or placebo infusion alongside corticosteroid and remdesivir treatments.
Main outcome measures: The primary endpoint was the time-to-event analysis difference in SWOV through day 28 between lenzilumab and placebo treatments, stratified by baseline CRP.
Results: SWOV was achieved in 152 (90%; 95% CI 85 to 94) lenzilumab and 144 (79%; 72 to 84) placebo-treated participants with baseline CRP <150 mg/L (HR: 2.54; 95% CI 1.46 to 4.41; p=0.0009) but not with CRP ≥150 mg/L (HR: 1.04; 95% CI 0.51 to 2.14; p=0.9058). A statistically significant interaction between CRP and lenzilumab treatment was observed (p=0.044). Grade ≥3 adverse events with lenzilumab were comparable to placebo in both CRP strata. No treatment-emergent serious adverse events were attributed to lenzilumab.
Conclusion: Hospitalised hypoxemic patients with COVID-19 with baseline CRP <150 mg/L derived the greatest clinical benefit from treatment with lenzilumab.
Trial registration number: NCT04351152; ClinicalTrials.gov.
Keywords: ARDS; COVID-19; Critical Care; Cytokine Biology; GM-CSF; Pneumonia; Respiratory Infection.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ZT has received research support from Humanigen, Inc, unrestricted education support from Gilead, ViiV, and Merck (all to the institution); CP is a paid consultant to Gilead; CFK has received research support grants (to the institution) from NIH, CDC, Gilead Sciences and ViiV; VCM has received investigator-initiated research grants (to the institution) and consultation fees (both unrelated to the current work) from Eli Lilly, Bayer, Gilead Sciences and ViiV; CD, DC, OA, AK and GC are employees of, or consultants to, Humanigen, Inc.; VMC and FC are third-party agency consultants to Humanigen.
Figures




References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous