

Transfer of congenital heart patients from paediatric to adult services in England
- PMID: 35794015
- PMCID: PMC9726960
- DOI: 10.1136/heartjnl-2022-321085
Transfer of congenital heart patients from paediatric to adult services in England
Abstract
Objective: This study assessed the transfer of patients from paediatric cardiac to adult congenital heart disease (ACHD) services in England and the factors impacting on this process.
Methods: This retrospective cohort study used a population-based linked data set (LAUNCHES QI data set: 'Linking Audit and National datasets in Congenital Heart Services for Quality Improvement') including all patients born between 1987 and 2000, recorded as having a congenital heart disease (CHD) procedure in childhood. Hospital Episode Statistics data identified transfer from paediatric to ACHD services between the ages of 16 and 22 years.
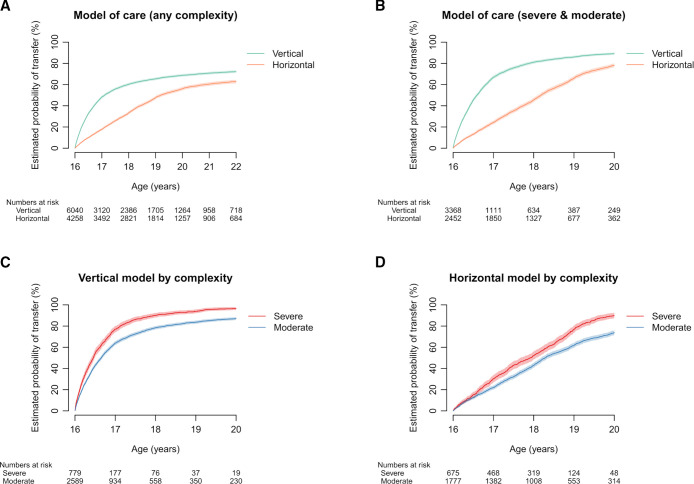
Results: Overall, 63.8% of a cohort of 10 298 patients transferred by their 22nd birthday. The estimated probability of transfer by age 22 was 96.5% (95% CI 95.3 to 97.7), 86.7% (95% CI 85.6 to 87.9) and 41.0% (95% CI 39.4 to 42.6) for severe, moderate and mild CHD, respectively. 166 patients (1.6%) died between 16 and 22 years; 42 of these (0.4%) died after age 16 but prior to transfer. Multivariable ORs in the moderate and severe CHD groups up to age 20 showed significantly lower likelihood of transfer among female patients (0.87, 95% CI 0.78 to 0.97), those with missing ethnicity data (0.31, 95% CI 0.18 to 0.52), those from deprived areas (0.84, 95% CI 0.72 to 0.98) and those with moderate (compared with severe) CHD (0.30, 95% CI 0.26 to 0.35). The odds of transfer were lower for the horizontal compared with the vertical care model (0.44, 95% CI 0.27 to 0.72). Patients who did not transfer had a lower probability of a further National Congenital Heart Disease Audit procedure between ages 20 and 30 compared with those who did transfer: 12.3% (95% CI 5.1 to 19.6) vs 32.5% (95% CI 28.7 to 36.3).
Conclusions: Majority of patients with moderate or severe CHD in England transfer to adult services. Patients who do not transfer undergo fewer elective CHD procedures over the following decade.
Keywords: Epidemiology; Health Care Economics and Organizations; Heart Defects, Congenital; Quality of Health Care.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Hernández-Madrid A, Paul T, Abrams D, et al. Arrhythmias in congenital heart disease: a position paper of the European Heart Rhythm Association (EHRA), Association for European Paediatric and Congenital Cardiology (AEPC), and the European Society of Cardiology (ESC) Working group on grown-up congenital heart disease, endorsed by HRS, PACES, APHRS, and SOLAECE. Europace 2018;20:1719–53. 10.1093/europace/eux380 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical