

Unexpected systolic anterior motion of the mitral valve-related hypoxemia during transurethral resection of the prostate under spinal anesthesia: a case report
- PMID: 35794519
- PMCID: PMC9258149
- DOI: 10.1186/s12871-022-01754-x
Unexpected systolic anterior motion of the mitral valve-related hypoxemia during transurethral resection of the prostate under spinal anesthesia: a case report
Abstract
Background: Dynamic obstruction of the left ventricular outflow tract resulting from systolic anterior motion of the mitral valve can be an unexpected cause of acute and severe perioperative hypotension in noncardiac surgery. We report a patient undergoing spinal anesthesia for transurethral resection of the prostate who experienced sudden hypoxemia caused by systolic anterior motion-induced mitral regurgitation but with a clinically picture simulating fluid overload.
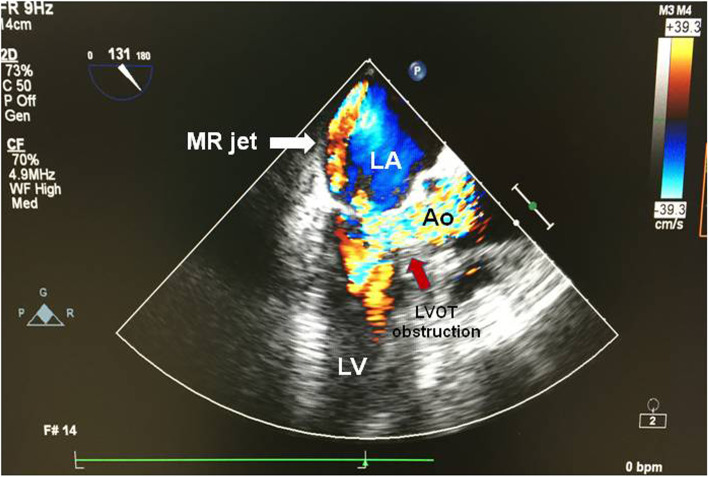
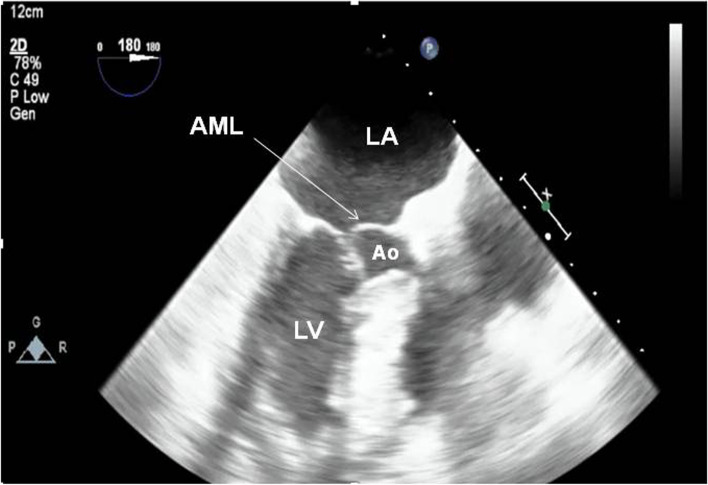
Case presentation: An 83-year-old man with a history of hypertension was scheduled for transurethral resection of the prostate. One hour after spinal anesthesia, he developed acute restlessness and dyspnea, with pink frothy sputum and progressive hypoxemia. Slight hypertension was noted, and an electrocardiogram showed atrial fibrillation with a rapid ventricular response. Furosemide and nitroglycerin were thus administered for suspected fluid overload or transurethral resection of the prostate syndrome; however, he then became severely hypotensive. After tracheal intubation, intraoperative transesophageal echocardiography was promptly performed, which revealed an empty hypercontractile left ventricle, significant mitral regurgitation and mosaic flow signal in the left ventricular outflow tract. Following aggressive fluid therapy, his hemodynamic changes stabilized. Repeat echocardiography in intensive care unit confirmed the presence of systolic anterior motion of the anterior mitral leaflet obstructing the left ventricular outflow tract. We speculate that pulmonary edema was induced by systolic anterior motion-associated mitral regurgitation and rapid atrial fibrillation, and the initial management had worsened his hypovolemia and provoked left ventricular outflow tract obstruction and hemodynamic instability.
Conclusions: Pulmonary edema caused by systolic anterior motion of the mitral valve can be difficult to clinically differentiate from that induced by fluid overload. Therefore, bedside echocardiography is paramount for timely diagnosis and prompt initiation of appropriate therapy in the perioperative care setting.
Keywords: Pulmonary edema; Spinal anesthesia; Systolic anterior motion; Transesophageal echocardiography; hypoxia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Sidebotham D, Legget M. The mitral valve. In: Sidebotham, editor. Practical and perioperative transesophageal echocardiography. Philadelphia: Butterworth-Heinemann; 2003. p. 149–50.
-
- Luckner G, Margreiter J, Jochberger S, Mayr V, Luger T, Voelckel W, et al. Systolic anterior motion of the mitral valve with left ventricular outflow tract obstruction: three cases of acute perioperative hypotension in noncardiac surgery. Anesth Analg. 2005;100:1594–1598. doi: 10.1213/01.ANE.0000152392.26910.5E. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
