

Composition and diversity analysis of the lung microbiome in patients with suspected ventilator-associated pneumonia
- PMID: 35794610
- PMCID: PMC9261066
- DOI: 10.1186/s13054-022-04068-z
Composition and diversity analysis of the lung microbiome in patients with suspected ventilator-associated pneumonia
Abstract
Background: Ventilator-associated pneumonia (VAP) is associated with high morbidity and health care costs, yet diagnosis remains a challenge. Analysis of airway microbiota by amplicon sequencing provides a possible solution, as pneumonia is characterised by a disruption of the microbiome. However, studies evaluating the diagnostic capabilities of microbiome analysis are limited, with a lack of alignment on possible biomarkers. Using bronchoalveolar lavage fluid (BALF) from ventilated adult patients suspected of VAP, we aimed to explore how key characteristics of the microbiome differ between patients with positive and negative BALF cultures and whether any differences could have a clinically relevant role.
Methods: BALF from patients suspected of VAP was analysed using 16s rRNA sequencing in order to: (1) differentiate between patients with and without a positive culture; (2) determine if there was any association between microbiome diversity and local inflammatory response; and (3) correctly identify pathogens detected by conventional culture.
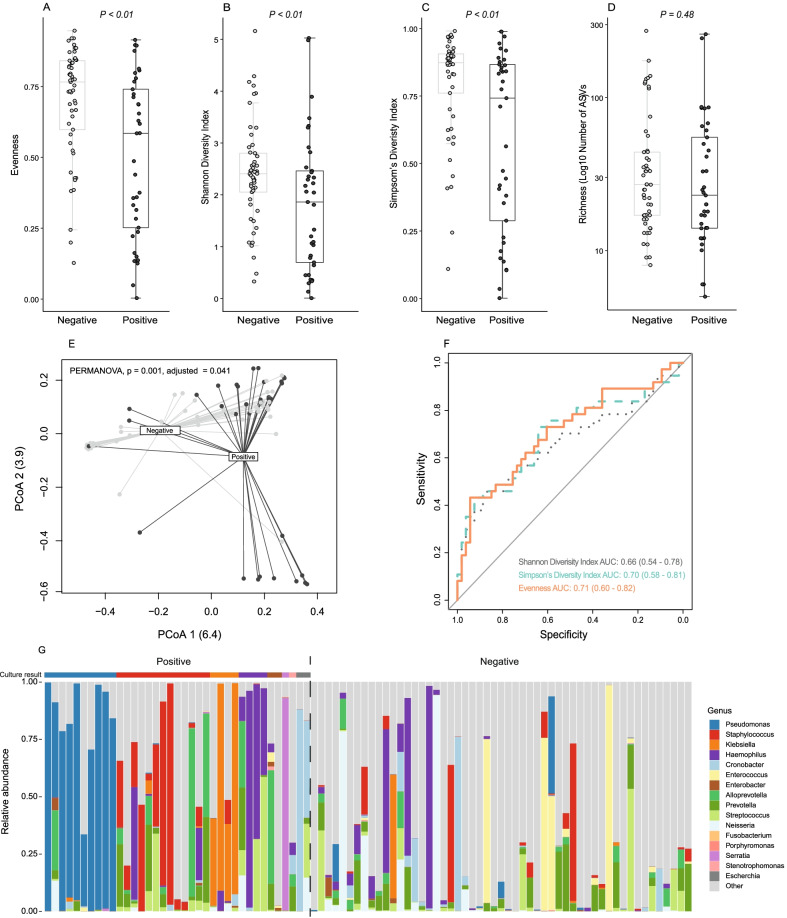
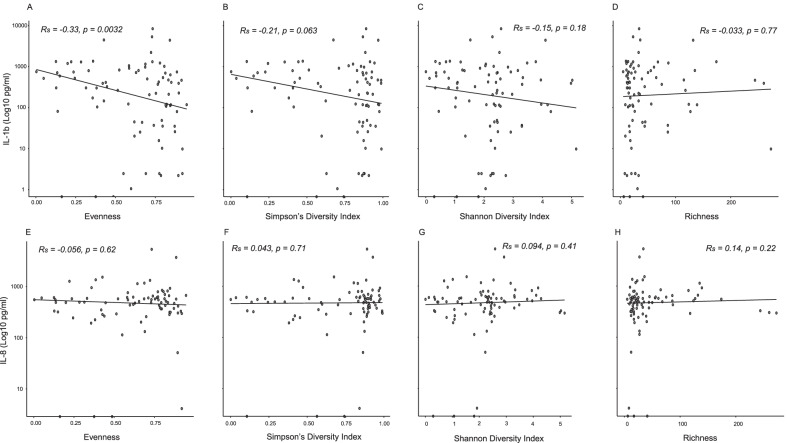
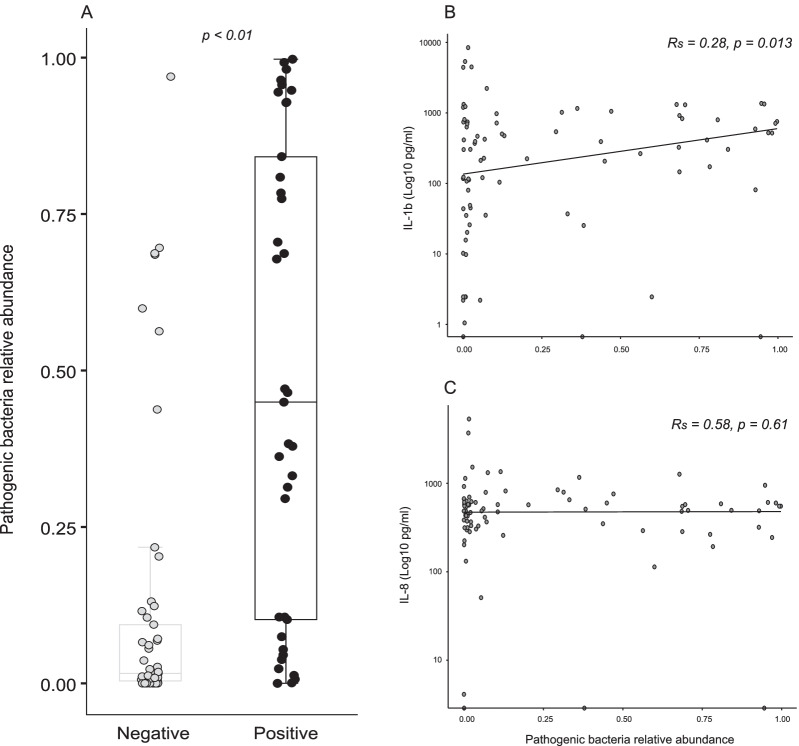
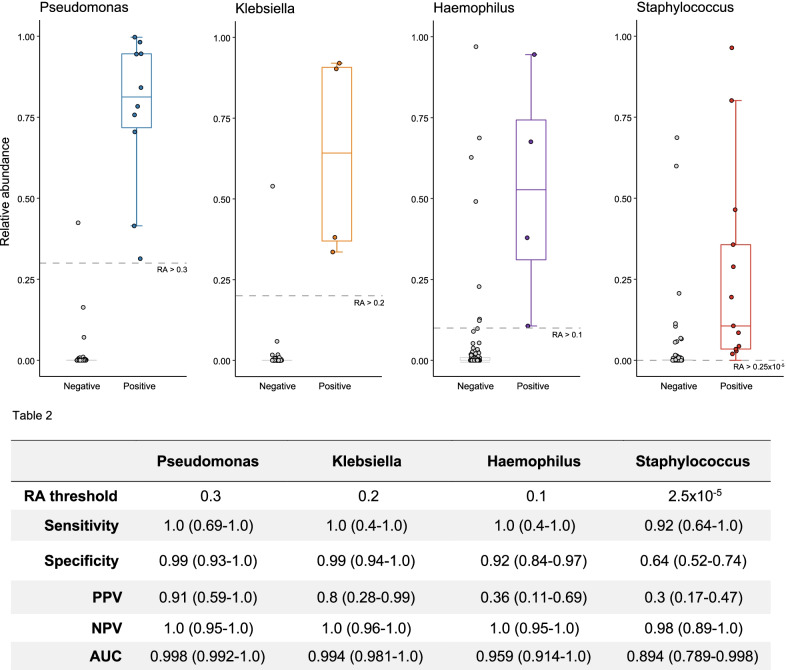
Results: Thirty-seven of 90 ICU patients with suspected VAP had positive cultures. Patients with a positive culture had significant microbiome dysbiosis with reduced alpha diversity. However, gross compositional variance was not strongly associated with culture positivity (AUROCC range 0.66-0.71). Patients with a positive culture had a significantly higher relative abundance of pathogenic bacteria compared to those without [0.45 (IQR 0.10-0.84), 0.02 (IQR 0.004-0.09), respectively], and an increased interleukin (IL)-1β was associated with reduced species evenness (rs = - 0.33, p < 0.01) and increased pathogenic bacteria presence (rs = 0.28, p = 0.013). Untargeted 16s rRNA pathogen detection was limited by false positives, while the use of pathogen-specific relative abundance thresholds showed better diagnostic accuracy (AUROCC range 0.89-0.998).
Conclusion: Patients with positive BALF culture had increased dysbiosis and genus dominance. An increased caspase-1-dependent IL-1b expression was associated with a reduced species evenness and increased pathogenic bacterial presence, providing a possible causal link between microbiome dysbiosis and lung injury development in VAP. However, measures of diversity were an unreliable predictor of culture positivity and 16s sequencing used agnostically could not usefully identify pathogens; this could be overcome if pathogen-specific relative abundance thresholds are used.
Keywords: Microbiome; Next-generation sequencing; Ventilator-associated pneumonia.
© 2022. The Author(s).
Conflict of interest statement
Dr Dominic Fenn has nothing to disclose. Dr Abdel-Aziz has nothing to disclose. Dr Pouline M. P. van Oort has nothing to disclose. Dr Paul Brinkman has nothing to disclose. Dr Waqar M. Ahmed has nothing to disclose. Dr Timothy Felton has nothing to disclose. Dr Antonio Artigas reports grants, personal fees and other from Grifols, grants from Fisher and Paykel, personal fees and other from Aerogen, other from Novartis, outside the submitted work. Dr Pedro Póvoa reports personal fees from MSD, personal fees from Gilead, outside the submitted work. Dr Ignacio Martin-Loeches has nothing to disclose. Dr Marcus J. Schultz has nothing to disclose. Dr Paul Dark has nothing to disclose. Dr Stephen J. Fowler has nothing to disclose. Dr Lieuwe D.J. Bos reports grants from the Dutch lung foundation (Young investigator grant), grants from the Dutch lung foundation and Health Holland (Public–Private Partnership grant), grants from the Dutch lung foundation (Dirkje Postma Award), grants from IMI COVID-19 initiative, grants from Amsterdam UMC fellowship, outside the submitted work. On behalf of the authors, I can confirm that there is no conflict of interest and that the manuscript has not been published elsewhere or under consideration by another journal. All the authors have approved the manuscript and agree with its submission to Critical Care.
Figures
References
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of america and the American thoracic society. Clin Infect Dis. 2016;63(5):e61–111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
