

Clinical Characteristics, Health Care Utilization, and Outcomes Among Patients in a Pilot Surveillance System for Invasive Mold Disease-Georgia, United States, 2017-2019
- PMID: 35794945
- PMCID: PMC9253885
- DOI: 10.1093/ofid/ofac215
Clinical Characteristics, Health Care Utilization, and Outcomes Among Patients in a Pilot Surveillance System for Invasive Mold Disease-Georgia, United States, 2017-2019
Abstract
Background: Invasive mold diseases (IMDs) cause severe illness, but public health surveillance data are lacking. We describe data collected from a laboratory-based, pilot IMD surveillance system.
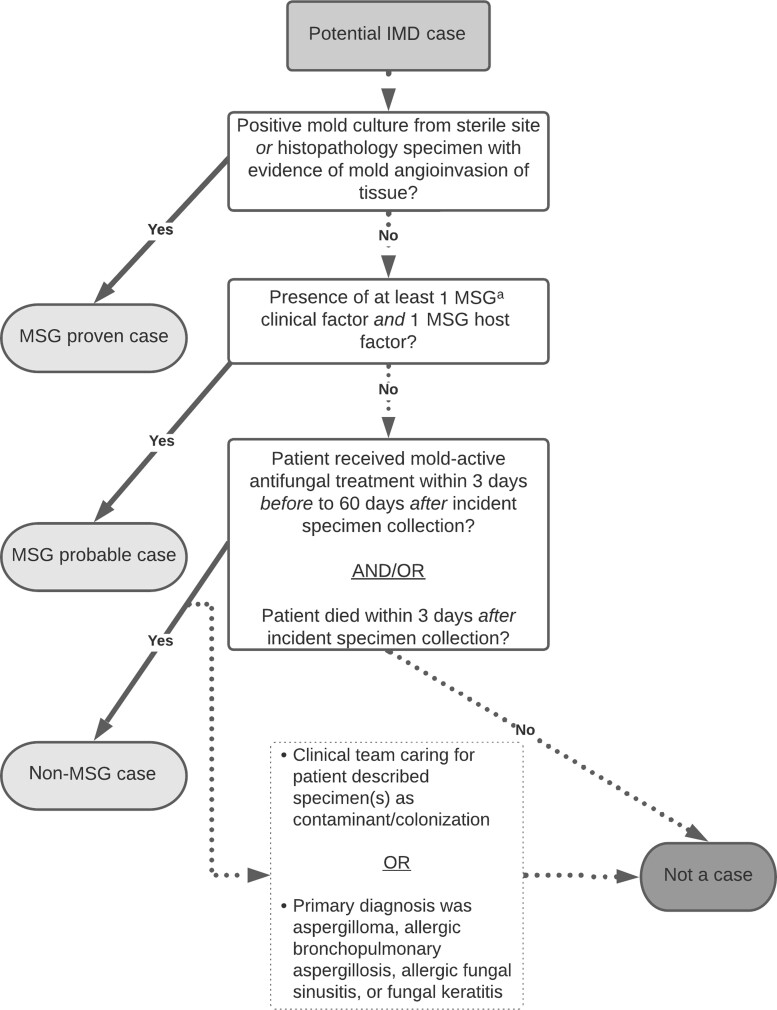
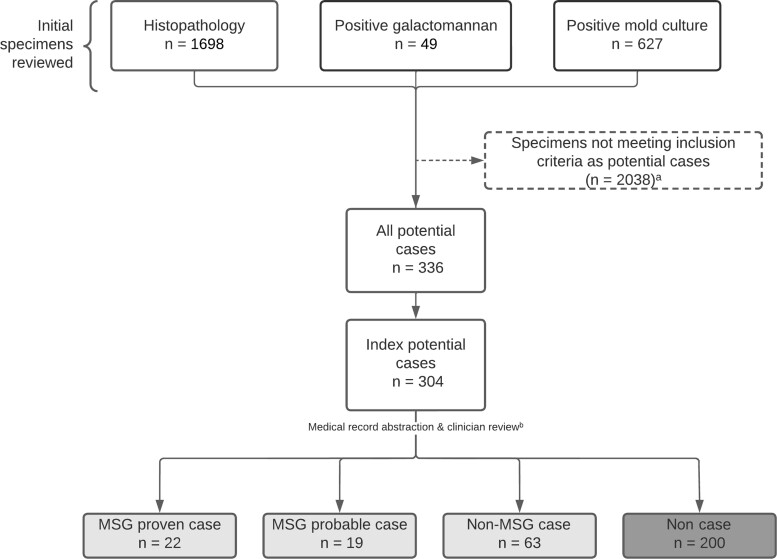
Methods: During 2017-2019, the Emerging Infections Program conducted active IMD surveillance at 3 Atlanta-area hospitals. We ascertained potential cases by reviewing histopathology, culture, and Aspergillus galactomannan results and classified patients as having an IMD case (based on European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group [MSG] criteria) or a non-MSG IMD case (based on the treating clinician's diagnosis and use of mold-active antifungal therapy). We described patient features and compared patients with MSG vs non-MSG IMD cases.
Results: Among 304 patients with potential IMD, 104 (34.2%) met an IMD case definition (41 MSG, 63 non-MSG). The most common IMD types were invasive aspergillosis (n = 66 [63.5%]), mucormycosis (n = 8 [7.7%]), and fusariosis (n = 4 [3.8%]); the most frequently affected body sites were pulmonary (n = 66 [63.5%]), otorhinolaryngologic (n = 17 [16.3%]), and cutaneous/deep tissue (n = 9 [8.7%]). Forty-five (43.3%) IMD patients received intensive care unit-level care, and 90-day all-cause mortality was 32.7%; these outcomes did not differ significantly between MSG and non-MSG IMD patients.
Conclusions: IMD patients had high mortality rates and a variety of clinical presentations. Comprehensive IMD surveillance is needed to assess emerging trends, and strict application of MSG criteria for surveillance might exclude over one-half of clinically significant IMD cases.
Keywords: antifungal drugs; invasive aspergillosis; invasive mold disease; mucormycosis; surveillance.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2022. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported cases. Clin Infect Dis 2005; 41:634–53. - PubMed
-
- Kontoyiannis DP, Marr KA, Park BJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001-2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) database. Clin Infect Dis 2010; 50:1091–100. - PubMed
-
- Lass-Flörl C, Cuenca-Estrella M. Changes in the epidemiological landscape of invasive mould infections and disease. J Antimicrob Chemother 2017; 72(Suppl 1):i5–11. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
