

Pulmonary vascular disease in pulmonary hypertension due to left heart disease: pathophysiologic implications
- PMID: 35796488
- PMCID: PMC9794188
- DOI: 10.1093/eurheartj/ehac184
Pulmonary vascular disease in pulmonary hypertension due to left heart disease: pathophysiologic implications
Abstract
Aims: Pulmonary hypertension (PH) and pulmonary vascular disease (PVD) are common and associated with adverse outcomes in left heart disease (LHD). This study sought to characterize the pathophysiology of PVD across the spectrum of PH in LHD.
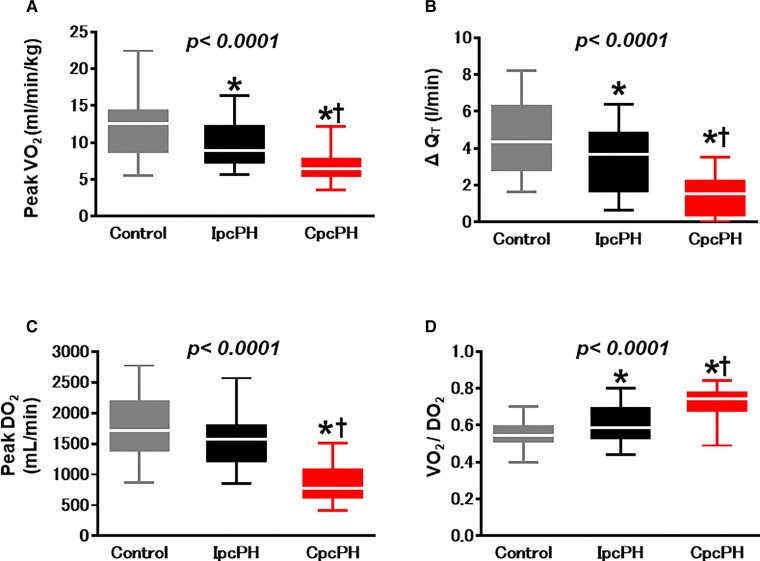
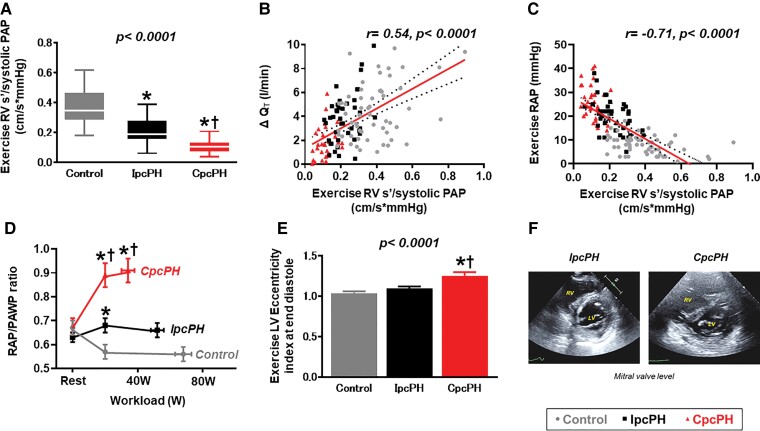
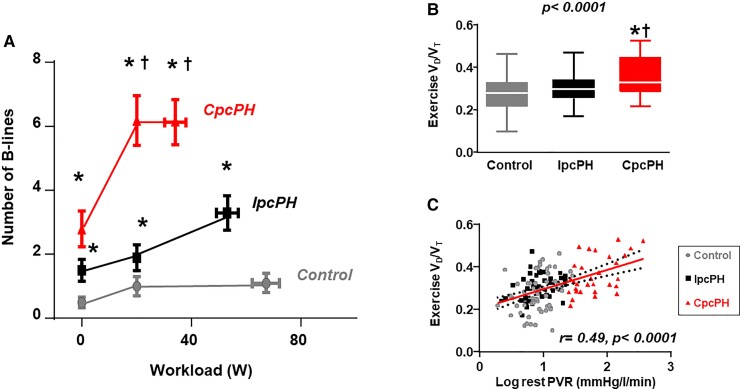
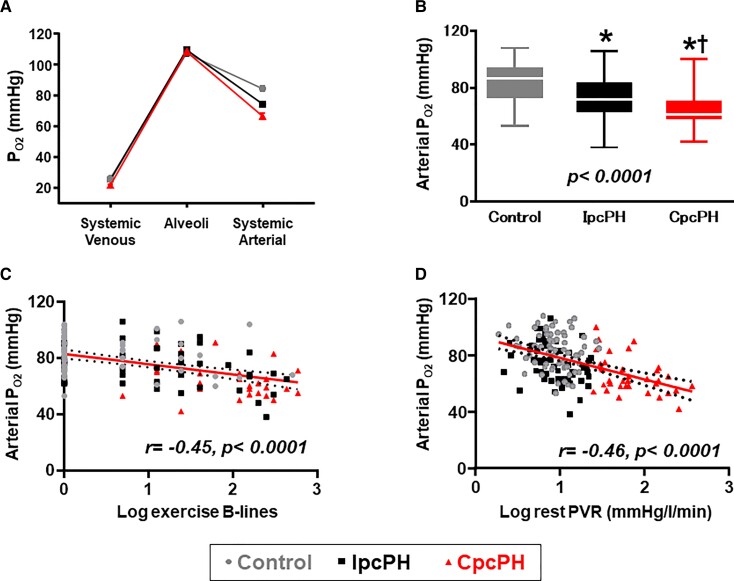
Methods and results: Patients with PH-LHD [mean pulmonary artery (PA) pressure >20 mmHg and PA wedge pressure (PAWP) ≥15 mmHg] and controls free of PH or LHD underwent invasive haemodynamic exercise testing with simultaneous echocardiography, expired air and blood gas analysis, and lung ultrasound in a prospective study. Patients with PH-LHD were divided into isolated post-capillary PH (IpcPH) and PVD [combined post- and pre-capillary PH (CpcPH)] based upon pulmonary vascular resistance (PVR <3.0 or ≥3.0 WU). As compared with controls (n = 69) and IpcPH-LHD (n = 55), participants with CpcPH-LHD (n = 40) displayed poorer left atrial function and more severe right ventricular (RV) dysfunction at rest. With exercise, patients with CpcPH-LHD displayed similar PAWP to IpcPH-LHD, but more severe RV-PA uncoupling, greater ventricular interaction, and more severe impairments in cardiac output, O2 delivery, and peak O2 consumption. Despite higher PVR, participants with CpcPH developed more severe lung congestion compared with both IpcPH-LHD and controls, which was associated lower arterial O2 tension, reduced alveolar ventilation, decreased pulmonary O2 diffusion, and greater ventilation-perfusion mismatch.
Conclusions: Pulmonary vascular disease in LHD is associated with a distinct pathophysiologic signature marked by greater exercise-induced lung congestion, arterial hypoxaemia, RV-PA uncoupling, ventricular interdependence, and impairment in O2 delivery, impairing aerobic capacity. Further study is required to identify novel treatments targeting the pulmonary vasculature in PH-LHD.
Keywords: Combined post- and pre-capillary pulmonary hypertension; Exercise haemodynamics; Heart failure; Left heart disease; Pulmonary hypertension; Pulmonary vascular resistance.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: none declared.
Figures

Comment in
-
Was Paul Wood wrong about pre-capillary pulmonary hypertension protecting against pulmonary congestion in left heart disease?Eur Heart J. 2022 Sep 21;43(36):3432-3434. doi: 10.1093/eurheartj/ehac176. Eur Heart J. 2022. PMID: 35796482 No abstract available.
-
Pulmonary haemodynamics and pulmonary congestion: where are we now?Eur Heart J. 2022 Nov 7;43(42):4515. doi: 10.1093/eurheartj/ehac499. Eur Heart J. 2022. PMID: 36104502 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
