

Vitamin D supplementation higher than 2000 IU/day compared to lower dose on maternal-fetal outcome: Systematic review and meta-analysis
- PMID: 35796578
- PMCID: PMC9274408
- DOI: 10.1177/17455057221111066
Vitamin D supplementation higher than 2000 IU/day compared to lower dose on maternal-fetal outcome: Systematic review and meta-analysis
Abstract
Introduction: Although vitamin D is widely known as an essential micronutrient during pregnancy, the exact supplementation dose to prevent maternal-fetal outcomes remains a question. This study aims to provide a systematic review and a meta-analysis of data from randomized controlled trial on > 2000 IU/day vitamin D supplementation compared to ⩽ 2000 IU/day; and ⩽ 2000 IU/day compared to placebo, on their effects on the incidence of preeclampsia, gestational diabetes mellitus, preterm birth, and differences on birth weight.
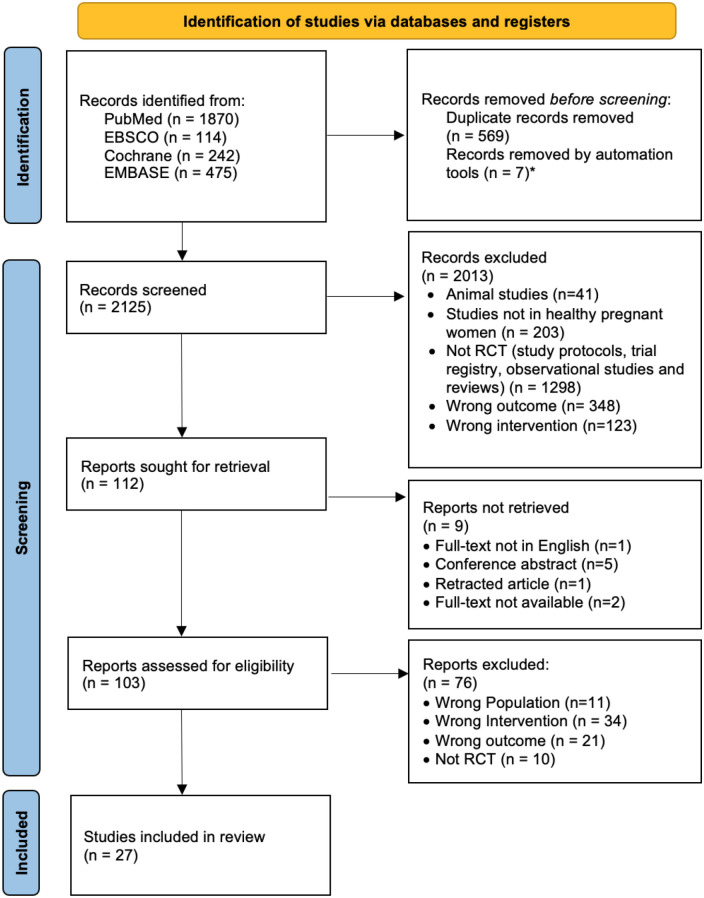
Methods: A systematic literature search on PubMed, EBSCO-MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials databases was carried out to evaluate randomized controlled trial studies on the effects of oral vitamin D > 2000 IU/day versus ⩽ 2000 IU/day; and ⩽ 2000 IU/day versus placebo, on preeclampsia, gestational diabetes mellitus, preterm birth and birth weight. Risk ratio, mean difference, and 95% confidence interval were calculated.
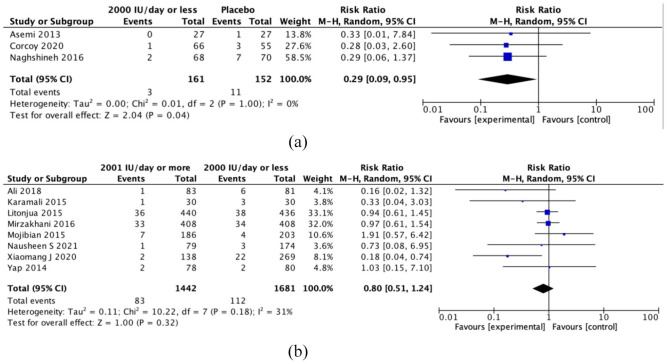
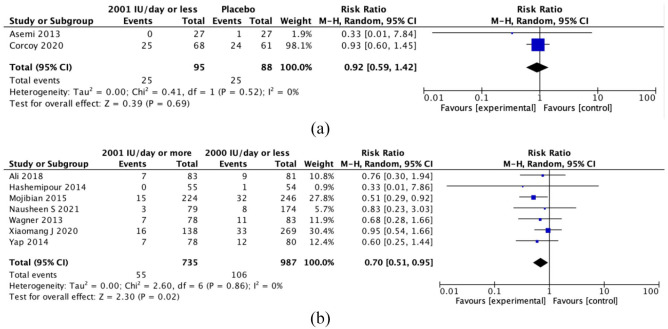
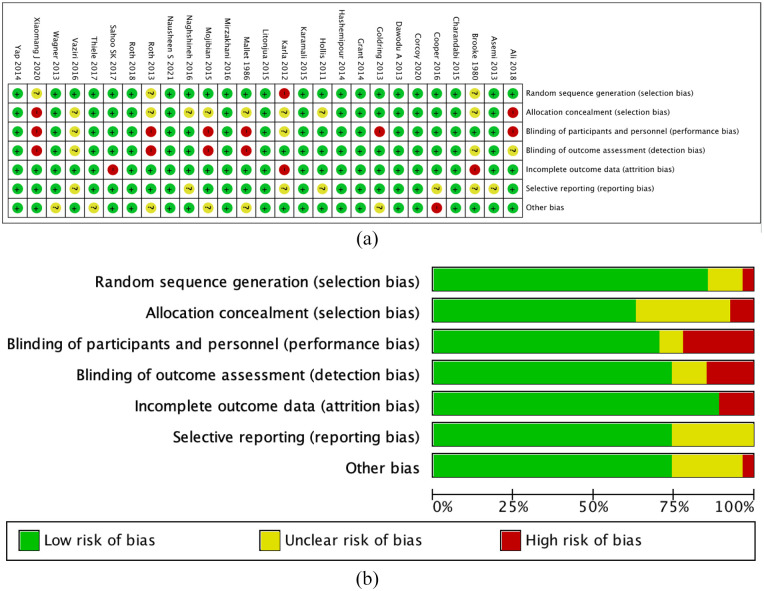
Results: There were a total of 27 randomized controlled trials selected. Maternal vitamin D supplementation > 2000 IU/day had a positive effect only on gestational diabetes mellitus (seven randomized controlled trials; risk ratio = 0.70, 95% confidence interval: 0.51-0.95, I2 = 0). Vitamin D supplementation ⩽ 2000 IU/day has reduced the risk of preeclampsia (three randomized controlled trials; risk ratio = 0.29, 95% confidence interval: 0.09-0.95, I2 = 0), with no significant difference when compared to > 2000 IU/day (eight randomized controlled trials; risk ratio = 0.80, 95% confidence interval: 0.51-1.24, I2 = 31). No difference in preterm birth risk and birth weight after vitamin D supplementation. The quality of evidence varies from moderate to very low certainty. The risk of preeclampsia and gestational diabetes mellitus after high-dose versus low-dose vitamin D supplementation was the ones with moderate certainty.
Conclusion: Vitamin D supplementation > 2000 IU/day might be important to reduce the risk of gestational diabetes mellitus. Lower dose vitamin D supplementation (⩽ 2000 IU/day) seemed adequate to reduce the risk of preeclampsia, with no significant difference compared to the higher dose.
Keywords: birth weight; gestational diabetes mellitus; preeclampsia; preterm birth; vitamin D.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
