

Disparities in Telemedicine Success and Their Association With Adverse Outcomes in Patients With Thoracic Cancer During the COVID-19 Pandemic
- PMID: 35797048
- PMCID: PMC9264040
- DOI: 10.1001/jamanetworkopen.2022.20543
Disparities in Telemedicine Success and Their Association With Adverse Outcomes in Patients With Thoracic Cancer During the COVID-19 Pandemic
Abstract
Importance: Disparities in access to telemedicine were identified at the onset of the COVID-19 pandemic, but the consequences of these disparities are not well characterized.
Objective: To investigate factors associated with successfully accessing and completing telemedicine visits and the association between telemedicine visit success and clinical outcomes among patients with thoracic cancer.
Design, setting, and participants: This retrospective cohort study included patients who attended outpatient visits at the thoracic oncology division of Johns Hopkins Medical Institute in Baltimore, Maryland, from March 1 to July 17, 2020.
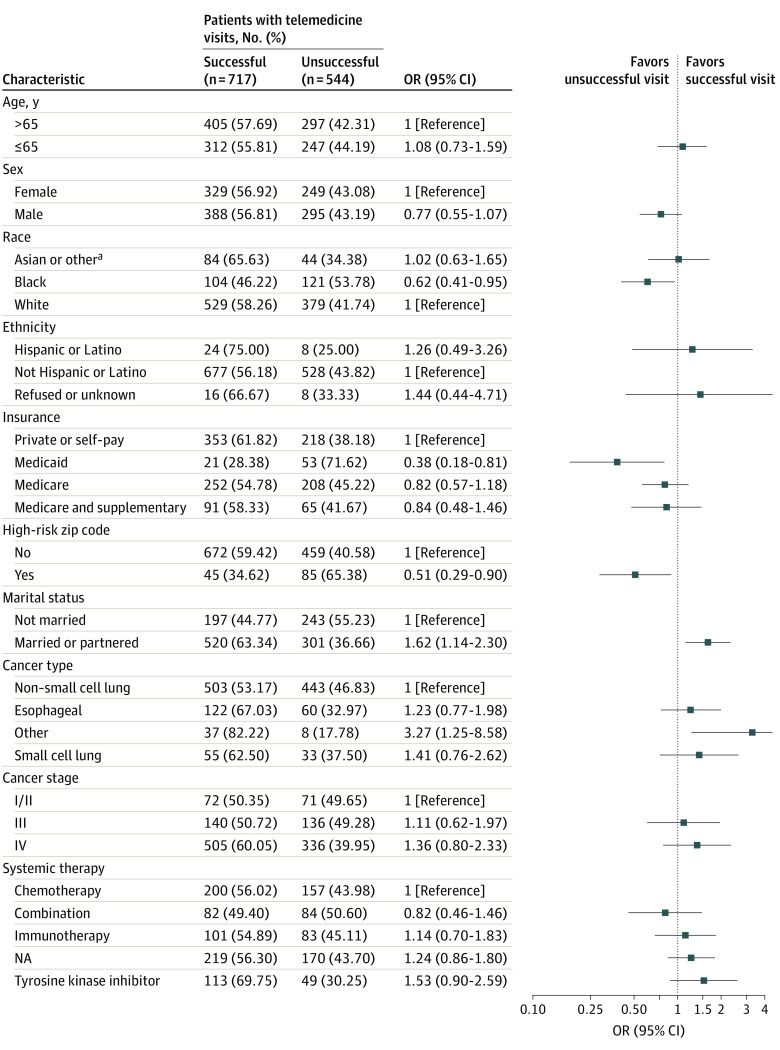
Main outcomes and measures: Associations of age, sex, race, ethnicity, insurance status, marital status, zip code, type of cancer, cancer stage, and type of therapy with telemedicine visit success (defined as completed visits with synchronous audio-video connection) and of visit success status with changes in therapy and odds of emergency department and urgent care visits, hospitalizations, and death were assessed using χ2 and Fisher exact tests and are reported as odds ratios (ORs).
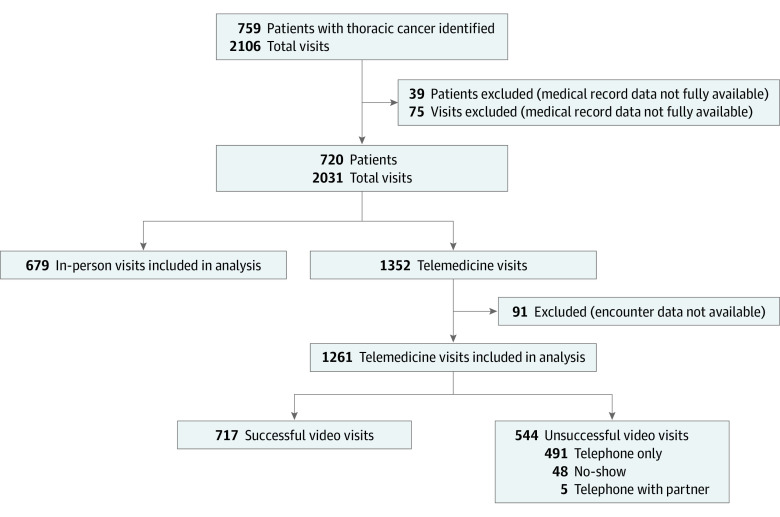
Results: A total of 720 patients and 1940 visits with complete data were included in the analysis; the median patient age was 65.7 years (range, 54.7-76.7 years), and 384 (53.33%) were male. Of the 1940 visits, 679 (35.00%) were in person and 1261 (65.00%) were telemedicine. Of the telemedicine visits, 717 (56.86%) were successful and 544 (43.14%) were unsuccessful. Patients who were Black (OR, 0.62; 95% CI, 0.41-0.95), had Medicaid (OR, 0.38; 95% CI, 0.18-0.81), or were from a zip code with an elevated risk of cancer mortality (OR, 0.51; 95% CI, 0.29-0.90) were less likely to have successful telemedicine visits than to have unsuccessful visits. Patients with at least 1 unsuccessful telemedicine visit had higher likelihood of an emergency department (OR, 2.73; 95% CI, 1.42-5.22) or urgent care (OR, 4.50; 95% CI, 2.41-8.41) visit or hospitalization (OR, 2.37; 95% CI, 1.17-4.80). Similarly, patients who had no successful telemedicine visits and for whom more than 1 telemedicine visit was scheduled had a higher likelihood of an emergency department (OR, 3.43; 95% CI 1.80-6.52) or urgent care (OR, 4.24; 95% CI 2.24-8.03) visit or hospitalization (OR, 4.19; 95% CI 2.17-8.10). Patients with all successful telemedicine visits (OR, 0.52; 95% CI, 0.30-0.90) or only 1, unsuccessful visit (OR, 0.32; 95% CI, 0.13-0.75) had lower odds of death compared with patients seen in-person only. Starting a new therapy was associated with lower odds of having a telemedicine visit vs an in-person visit (OR, 0.49; 95% CI, 0.37-0.64) and higher odds of a successful telemedicine visit vs an unsuccessful telemedicine visit (OR, 1.90; 95% CI, 1.28-2.82).
Conclusions and relevance: In this cohort study, patients with thoracic cancer who were Black, had Medicaid, or were from a zip code with a high risk of cancer mortality had increased odds of unsuccessful telemedicine visits compared with their counterparts and unsuccessful telemedicine visits were associated with worse clinical outcomes compared with successful visits. These findings suggest that more work is needed to improve telemedicine access for disadvantaged patients.
Conflict of interest statement
Figures
Comment in
-
Current and Future Questions for Telemedicine Research in Oncology-Moving Beyond Feasibility.JAMA Netw Open. 2022 Jul 1;5(7):e2220550. doi: 10.1001/jamanetworkopen.2022.20550. JAMA Netw Open. 2022. PMID: 35797052 No abstract available.
References
-
- European Society for Medical Oncology . ESMO management and treatment adapted recommendations in the COVID-19 era: lung cancer. Accessed November 1, 2021. https://www.esmo.org/guidelines/cancer-patient-management-during-the-cov...
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
