

Race, rituximab, and relapse in TTP
- PMID: 35797471
- PMCID: PMC9710186
- DOI: 10.1182/blood.2022016640
Race, rituximab, and relapse in TTP
Abstract
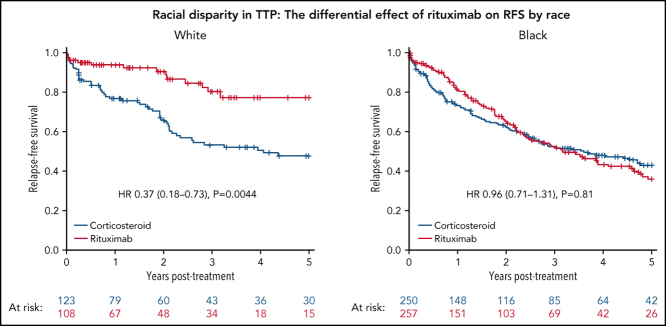
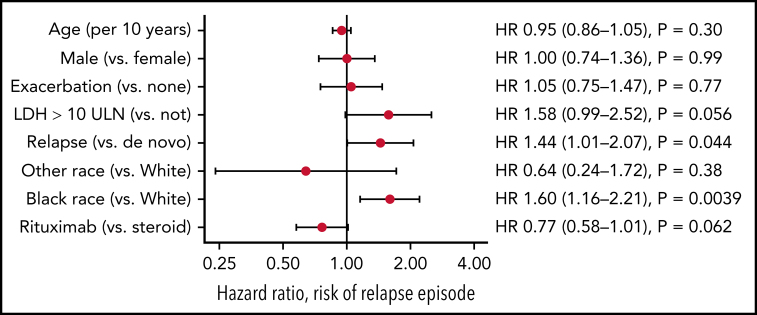
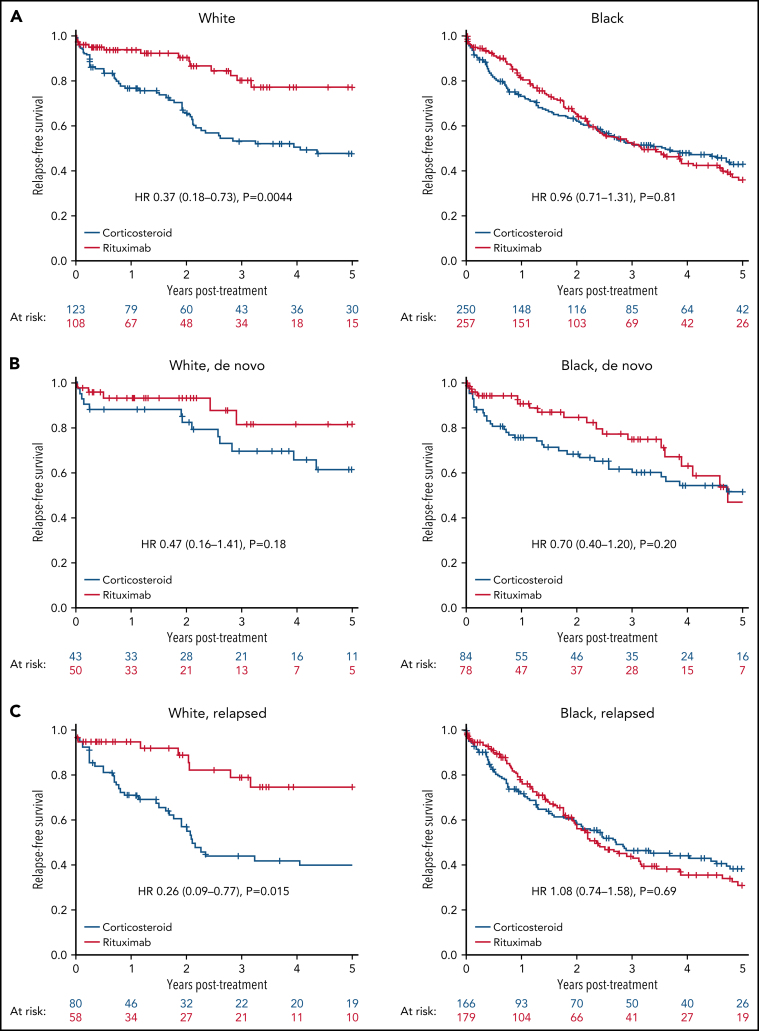
Immune-mediated thrombotic thrombocytopenic purpura (iTTP) is characterized by recurring episodes of thrombotic microangiopathy, causing ischemic organ impairment. Black patients are overrepresented in iTTP cohorts in the United States, but racial disparities in iTTP outcome and response to therapy have not been studied. Using the United States Thrombotic Microangiopathies Consortium iTTP Registry, we evaluated the impact of race on mortality and relapse-free survival (RFS) in confirmed iTTP in the United States from 1995 to 2020. We separately examined the impact of rituximab therapy and presentation with newly diagnosed (de novo) or relapsed iTTP on RFS by race. A total of 645 participants with 1308 iTTP episodes were available for analysis. Acute iTTP mortality did not differ by race. When all episodes of iTTP were included, Black race was associated with shorter RFS (hazard ratio [HR], 1.60; 95% CI, 1.16-2.21); the addition of rituximab to corticosteroids improved RFS in White (HR, 0.37; 95% CI, 0.18-0.73) but not Black patients (HR, 0.96; 95% CI, 0.71-1.31). In de novo iTTP, rituximab delayed relapse, but Black patients had shorter RFS than White patients, regardless of treatment. In relapsed iTTP, rituximab significantly improved RFS in White but not Black patients. Race affects overall relapse risk and response to rituximab in iTTP. Black patients may require closer monitoring, earlier retreatment, and alternative immunosuppression after rituximab treatment. How race, racism, and social determinants of health contribute to the disparity in relapse risk in iTTP deserves further study.
© 2022 by The American Society of Hematology.
Figures
Comment in
-
iTPP: nature vs nurture?Blood. 2022 Sep 22;140(12):1329-1330. doi: 10.1182/blood.2022017562. Blood. 2022. PMID: 36136362 No abstract available.
References
-
- Furlan M, Robles R, Galbusera M, et al. von Willebrand factor-cleaving protease in thrombotic thrombocytopenic purpura and the hemolytic-uremic syndrome. N Engl J Med. 1998;339(22):1578–1584. - PubMed
-
- Rock GA, Shumak KH, Buskard NA, et al. Canadian Apheresis Study Group Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. N Engl J Med. 1991;325(6):393–397. - PubMed
-
- Scully M, Cataland SR, Peyvandi F, et al. Caplacizumab treatment for acquired thrombotic thrombocytopenic purpura. N Engl J Med. 2019;380(4):335–346. https://doi.org/10.1056/NEJMoa1806311. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
