

Effects of immune-mediated inflammatory diseases on cardiovascular diseases in patients with type 2 diabetes: a nationwide population-based study
- PMID: 35798796
- PMCID: PMC9262934
- DOI: 10.1038/s41598-022-15436-8
Effects of immune-mediated inflammatory diseases on cardiovascular diseases in patients with type 2 diabetes: a nationwide population-based study
Abstract
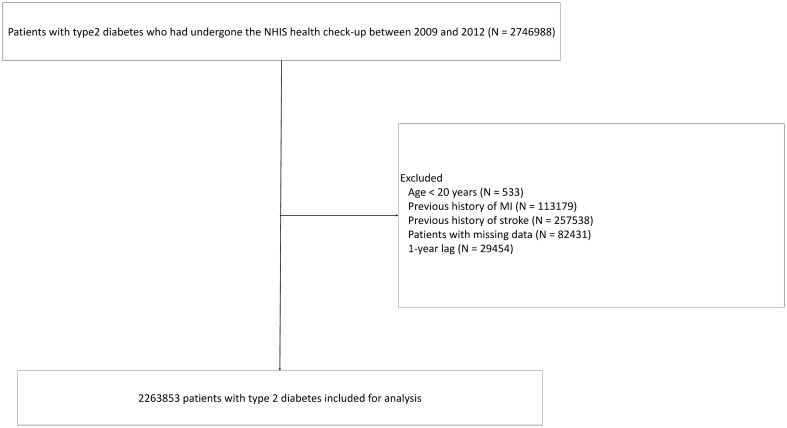
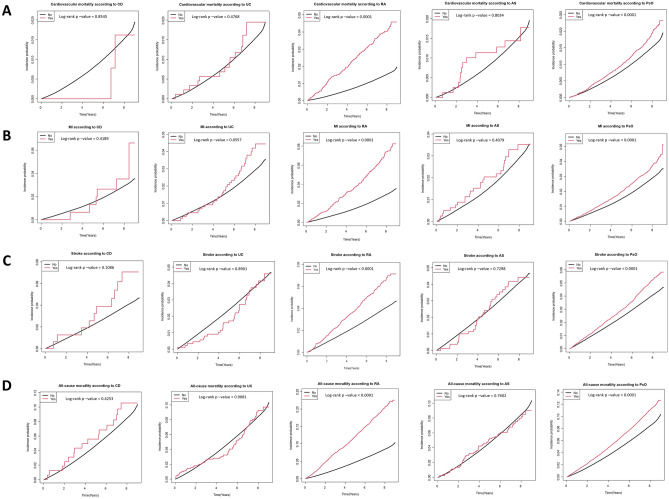
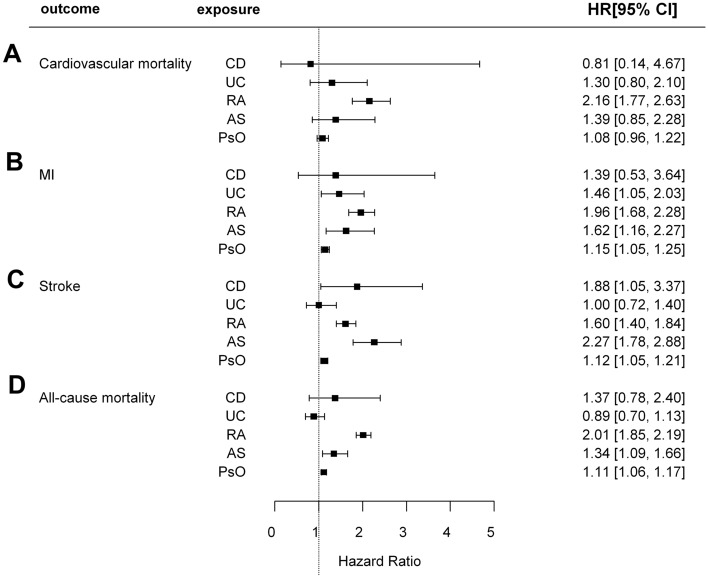
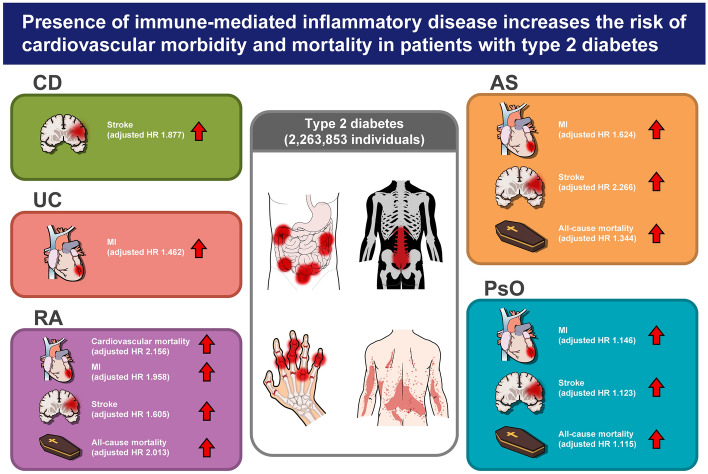
Both type 2 diabetes and immune-mediated inflammatory diseases (IMIDs), such as Crohn's disease (CD), ulcerative colitis, rheumatoid arthritis (RA), ankylosing spondylitis (AS), and psoriasis (PsO) are risk factors of cardiovascular disease. Whether presence of IMIDs in patients with type 2 diabetes increases their cardiovascular risk remains unclear. We aimed to investigate the risk of cardiovascular morbidity and mortality in patients with type 2 diabetes and IMIDs. Patients with type 2 diabetes without cardiovascular disease were retrospectively enrolled from nationwide data provided by the Korean National Health Insurance Service. The primary outcome was cardiovascular mortality, and the secondary outcomes were myocardial infarction (MI), stroke, and all-cause mortality. Inverse probability of treatment weighting (IPTW)-adjusted Cox proportional hazard regression analysis was performed to estimate the hazard ratios (HRs) and 95% confidence intervals (95% CIs) for each IMID. Overall 2,263,853 patients with type 2 diabetes were analyzed. CD was associated with a significantly higher risk of stroke (IPTW-adjusted HR: 1.877 [95%CI 1.046, 3.367]). UC was associated with a significantly higher risk of MI (1.462 [1.051, 2.032]). RA was associated with a significantly higher risk of cardiovascular mortality (2.156 [1.769, 2.627]), MI (1.958 [1.683, 2.278]), stroke (1.605 [1.396, 1.845]), and all-cause mortality (2.013 [1.849, 2.192]). AS was associated with a significantly higher risk of MI (1.624 [1.164, 2.266]), stroke (2.266 [1.782, 2.882]), and all-cause mortality (1.344 [1.089, 1.658]). PsO was associated with a significantly higher risk of MI (1.146 [1.055, 1.246]), stroke (1.123 [1.046, 1.205]) and all-cause mortality (1.115 [1.062, 1.171]). In patients with type 2 diabetes, concomitant IMIDs increase the risk of cardiovascular morbidity and mortality. Vigilant surveillance for cardiovascular disease is needed in patients with type 2 diabetes and IMIDs.
© 2022. The Author(s).
Conflict of interest statement
Dr. Chun received a grant given by Eisai Co. All other authors disclose that they have no financial, professional, or personal conflicts related to this publication.
Figures
References
-
- Low-Wang CC, Hess CN, Hiatt WR, Goldfine AB. Clinical update: Cardiovascular disease in diabetes mellitus: Atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus: Mechanisms, management, and clinical considerations. Circulation. 2016;133:2459–2502. doi: 10.1161/circulationaha.116.022194. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
