

Over- and under-prescribing, and their association with functional disability in older patients at risk of further decline in Germany - a cross-sectional survey conducted as part of a randomised comparative effectiveness trial
- PMID: 35799113
- PMCID: PMC9260981
- DOI: 10.1186/s12877-022-03242-w
Over- and under-prescribing, and their association with functional disability in older patients at risk of further decline in Germany - a cross-sectional survey conducted as part of a randomised comparative effectiveness trial
Abstract
Background: Older patients at risk of functional decline are frequently affected by polypharmacy. This is associated with a further loss of independence. However, a relationship between functional disability and medications, such as 'Potentially Inappropriate Medications' (PIMs) and 'Potential Prescribing Omissions' (PPOs), as itemised for (de) prescribing in practice-orientated medication lists, has yet to be established.
Methods: As part of a randomised comparative effectiveness trial, LoChro, we conducted a cross-sectional analysis of the association between PIMs and PPOs measured using the 'Screening Tool of Older Persons' Prescription Criteria / Screening Tool To Alert to Right Treatment' (STOPP/START) Version 2, with functional disability assessed using the 'World Health Organization Disability Assessment Schedule 2.0' (WHODAS). Individuals aged 65 and older at risk of loss of independence were recruited from the inpatient and outpatient departments of the local university hospital. Multiple linear regression analysis was used to model the potential prediction of functional disability using the numbers of PIMs and PPOs, adjusted for confounders including multimorbidity.
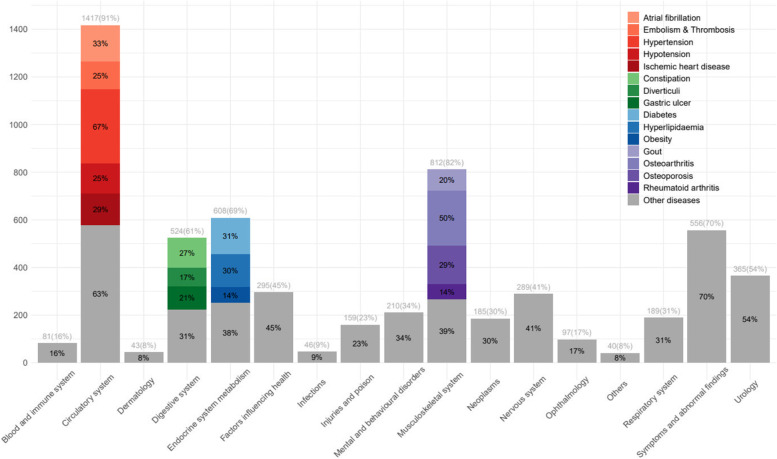
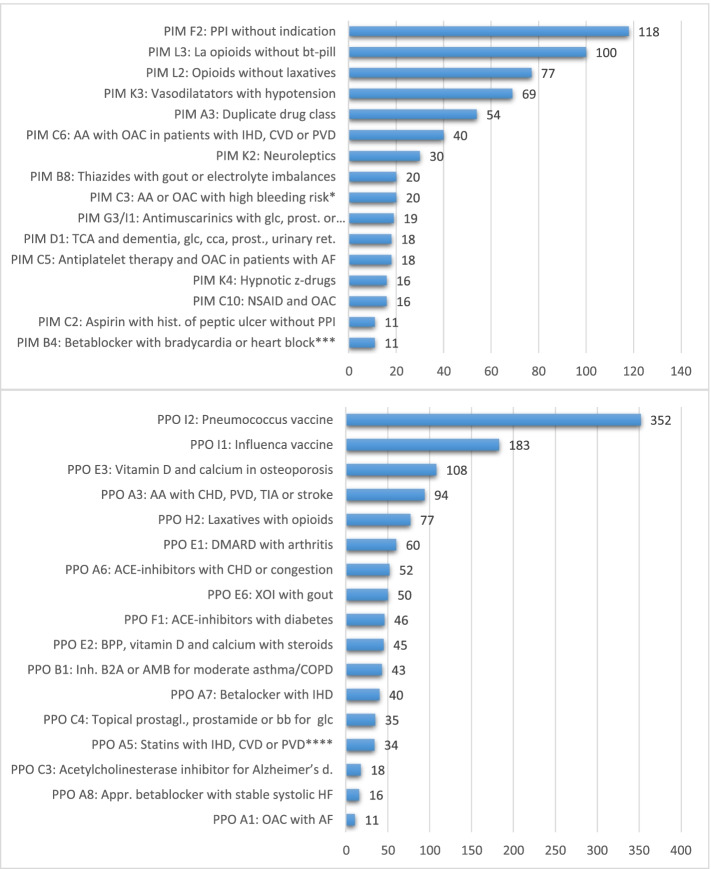
Results: Out of 461 patients, both the number of PIMs and the number of PPOs were significantly associated with an increase in WHODAS-score (Regression coefficients B 2.7 [95% confidence interval: 1.5-3.8] and 1.5 [95% confidence interval: 0.2-2.7], respectively). In WHODAS-score prediction modelling the contribution of the number of PIMs exceeded the one of multimorbidity (standardised coefficients beta: PIM 0.20; multimorbidity 0.13; PPO 0.10), whereas no significant association between the WHODAS-score and the number of medications was seen. 73.5 % (339) of the participants presented with at least one PIM, and 95.2% (439) with at least one PPO. The most common PIMs were proton pump inhibitors and analgesic medication, with frequent PPOs being pneumococcal and influenza vaccinations, as well as osteoporosis prophylaxis.
Conclusions: The results indicate a relationship between inappropriate prescribing, both PIMs and PPOs, and functional disability, in older patients at risk of further decline. Long-term analysis may help clarify whether these patients benefit from interventions to reduce PIMs and PPOs.
Keywords: functional disability; inappropriate prescribing; multimorbidity; polypharmacy; potential prescribing omissions; potentially inappropriate medications.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Khezrian M, McNeil CJ, Murray AD, Myint PK. An overview of prevalence, determinants and health outcomes of polypharmacy. Ther Adv Drug Saf. 2020;12 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7294476/. - PMC - PubMed
-
- Montiel-Luque A, Núñez-Montenegro AJ, Martín-Aurioles E, Canca-Sánchez JC, Toro-Toro MC, González-Correa JA. Medication-related factors associated with health-related quality of life in patients older than 65 years with polypharmacy. PLoS One. 2017;12(2):e0171320. doi: 10.1371/journal.pone.0171320. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
