

Comparison of the prevalence of kidney disease by proteinuria and decreased estimated glomerular filtration rate determined using three creatinine-based equations among patients admitted on medical wards of Masaka Regional Referral Hospital in Uganda: a prospective study
- PMID: 35799132
- PMCID: PMC9264612
- DOI: 10.1186/s12882-022-02865-w
Comparison of the prevalence of kidney disease by proteinuria and decreased estimated glomerular filtration rate determined using three creatinine-based equations among patients admitted on medical wards of Masaka Regional Referral Hospital in Uganda: a prospective study
Abstract
Background: Despite estimated glomerular filtration rate (eGFR) being the best marker for kidney function, there are no studies in sub-Saharan Africa comparing the performance of various equations used to determine eGFR. We compared prevalence of kidney disease determined by proteinuria of ≥ + 1 and or kidney disease improving global outcomes (KDIGO) eGFR criteria of < 60 ml/minute/1.73m2 determined using three creatinine-based equations among patients admitted on medical ward of Masaka Regional Referral Hospital.
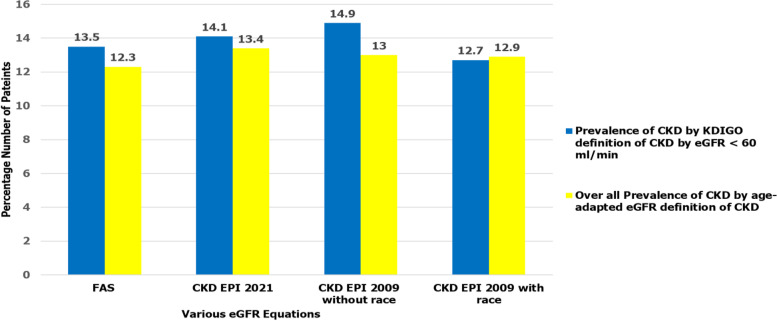
Methods: This was a prospective study conducted among adult patients admitted on medical wards between September 2020 to March 2021. Spot urine samples were collected to assess for proteinuria and blood samples were collected to assess serum creatinine levels. Kidney disease was defined as proteinuria of ≥ 1 + on spot urine dipstick and or KDIGO eGFR criteria of < 60 ml/minute/1.73m2. Estimated glomerular filtration rate was calculated using three creatinine-based equations: a) Full Age Spectrum equation (FAS), b) chronic kidney disease-Epidemiology collaboration (CKD-EPI) 2021 equation, c) CKD EPI 2009 (without and with race factor) equation. CKD was determined after followed up at 90 days post enrollment to determine the chronicity of proteinuria of ≥ + 1 and or KDIGO eGFR criteria of < 60mls /minute/1.73m2. We also compared prevalence of CKD determined by KDIGO eGFR criteria of < 60mls /minute/1.73m2 vs age adapted eGFR threshold criteria for defining CKD.
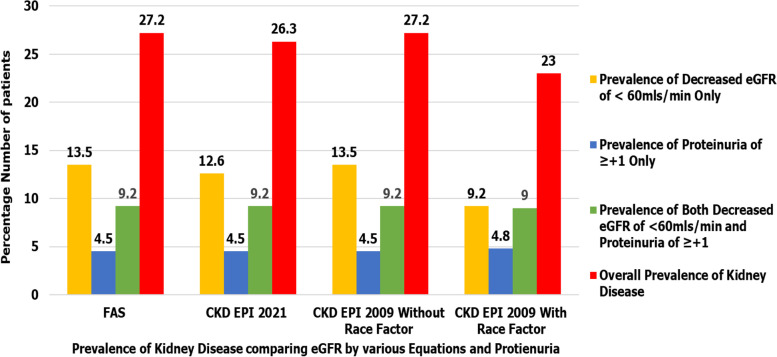
Results: Among the 357 patients enrolled in the study, KDIGO eGFR criteria of < 60mls / minute determined using FAS and CKD-EPI 2009 without race factor equations and or proteinuria of ≥ + 1 showed the highest overall prevalence of kidney disease at 27.2%. Prevalence of confirmed CKD at 90 days was highest with proteinuria ≥ + 1 and or KDIGO eGFR criteria of < 60mls/min determined using CKD EPI 2009 without race factor Equation (15.1%).
Conclusions: Use of KDIGO eGFR criteria of < 60mls / minute /1.73m2 using FAS and CKD-EPI 2009 without race equations identifies the largest number of patients with CKD. Health care systems in sub-Saharan Africa should calculate eGFR using FAS equations or CKD-EPI 2009 without race equations during basic screening and management protocols.
Keywords: Comparison of prevalence of kidney disease; Estimated glomerular filtration rate equations; Kidney disease.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Low estimated glomerular filtration rate and proteinuria among adult diabetic patients in a tertiary hospital in Eastern Uganda - a cross-sectional study.BMC Nephrol. 2024 Sep 27;25(1):319. doi: 10.1186/s12882-024-03764-y. BMC Nephrol. 2024. PMID: 39333932 Free PMC article.
-
The New Creatinine-Based Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) 2021 Equation: Potential Impact on Screening for Chronic Kidney Disease in an Asymptomatic Black African Population.J Appl Lab Med. 2024 May 2;9(3):502-511. doi: 10.1093/jalm/jfae002. J Appl Lab Med. 2024. PMID: 38384166
-
Performance of creatinine- or cystatin C-based equations to estimate glomerular filtration rate in sub-Saharan African populations.Kidney Int. 2019 May;95(5):1181-1189. doi: 10.1016/j.kint.2018.11.045. Epub 2019 Mar 12. Kidney Int. 2019. PMID: 30910379
-
GFR estimation: from physiology to public health.Am J Kidney Dis. 2014 May;63(5):820-34. doi: 10.1053/j.ajkd.2013.12.006. Epub 2014 Jan 28. Am J Kidney Dis. 2014. PMID: 24485147 Free PMC article. Review.
-
Impact of the choice of biomarkers and equations to estimate kidney function on the epidemiology of chronic kidney disease.Curr Opin Nephrol Hypertens. 2025 Jul 1;34(4):336-345. doi: 10.1097/MNH.0000000000001085. Epub 2025 May 16. Curr Opin Nephrol Hypertens. 2025. PMID: 40387074 Review.
Cited by
-
Use of hospital services by patients with chronic conditions in sub-Saharan Africa: a systematic review and meta-analysis.Bull World Health Organ. 2023 Sep 1;101(9):558-570G. doi: 10.2471/BLT.22.289597. Epub 2023 Jul 5. Bull World Health Organ. 2023. PMID: 37638357 Free PMC article.
-
Comparison and evaluation of the 2009 and 2021 chronic kidney disease-epidemiological collaboration equations among Jordanian patients with type 2 diabetes mellitus.Acta Diabetol. 2024 Feb;61(2):169-180. doi: 10.1007/s00592-023-02191-z. Epub 2023 Oct 8. Acta Diabetol. 2024. PMID: 37805971
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392(10159):1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Kellum JA, Lameire N, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, et al. Kidney disease: improving global outcomes (KDIGO) acute kidney injury work group KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1–138. doi: 10.1038/kisup.2012.1. - DOI
-
- Kiggundu B, Kalyesubula R, Ssinabulya i, Achilles K, Emmanuel S. Chronic Kidney Disease among Hypertensive Patients Attending a National Referral Hospital in Uganda. J Urol Renal Dis. 2017;2017(06):144. 10.29011/2575-7903.000044.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
