

Epidemiological Characteristics of Primary Liver Cancer in Mainland China From 2003 to 2020: A Representative Multicenter Study
- PMID: 35800051
- PMCID: PMC9253580
- DOI: 10.3389/fonc.2022.906778
Epidemiological Characteristics of Primary Liver Cancer in Mainland China From 2003 to 2020: A Representative Multicenter Study
Abstract
Background: The contribution of hepatitis B virus (HBV) and hepatitis C virus (HCV) to primary liver cancer (PLC) and their association with cancer aggressiveness remains uncertain in China, a country with half of global PLC. We aimed to characterize this using data from four representative medical centers.
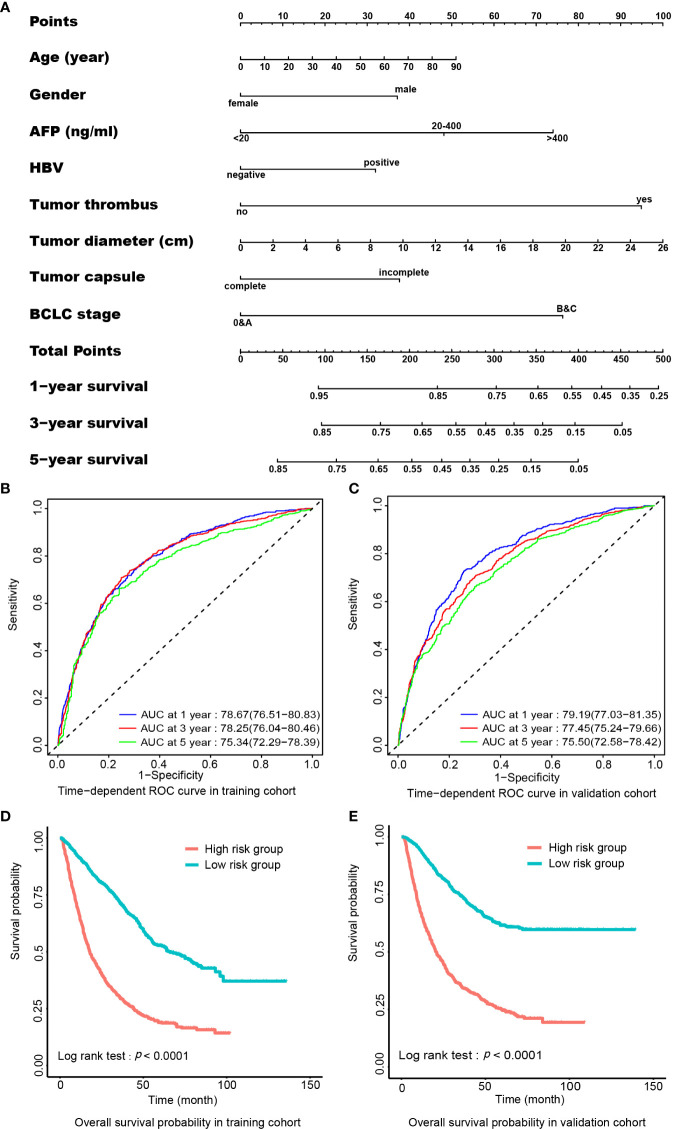
Methods: In total, 15,801 PLC patients were enrolled from the centers distributed in Easter5n, Southern, Northern, and Western China from 2003 to 2020. Of those, 7585 with curative surgery were involved in survival analysis. A nomogram was constructed using preoperative parameters to predict postoperative survival.
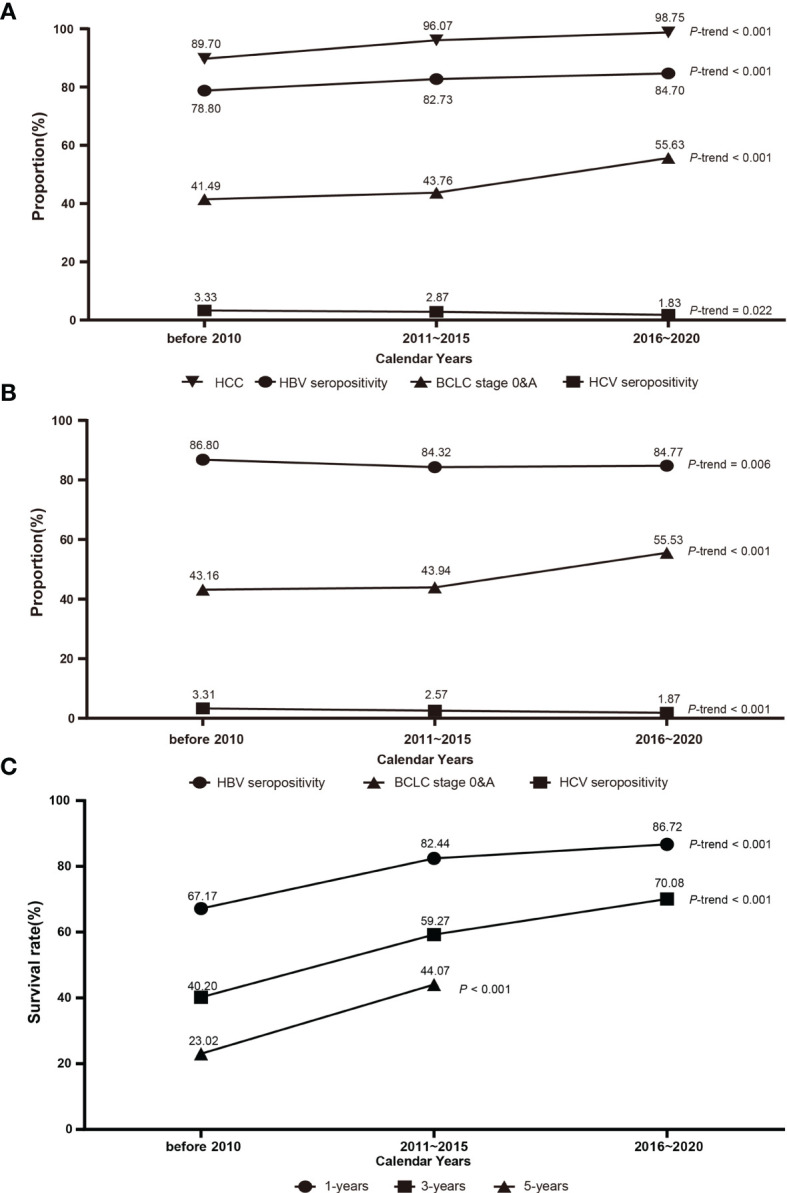
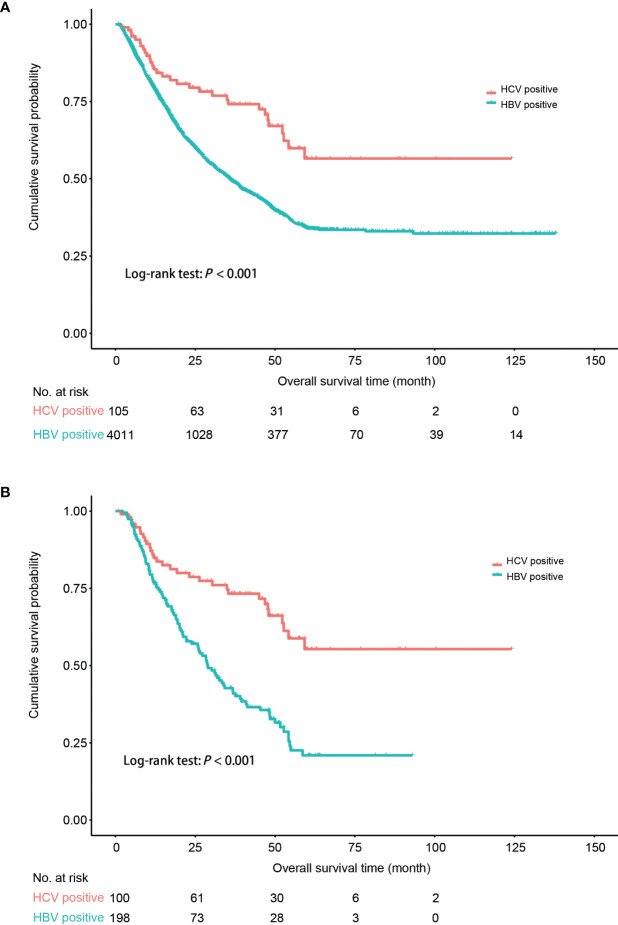
Results: Hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma, and combined hepatocellular cholangiocarcinoma accounted for 93.0%, 4.3%, and 1.6% in PLC, respectively. The seropositivities of HBV and HCV were 84.4% and 3.2% in HCC, respectively. The seropositivity of anti-HCV antibody was significantly higher in HBV-negative than in HBV-positive HCC patients (13.2% vs. 1.1%). Compared to HCV-positive HCC (HCV-HCC), HBV-positive HCC (HBV-HCC) was associated with 12-year earlier onset, higher proportions of males, high α-fetoprotein, large tumor size, advanced Barcelona Clinic Liver Cancer (BCLC) stage, and vascular tumor thrombus. The proportions of HCC and HBV seropositivity increased, whereas that of anti-HCV decreased, from 2003 to 2020. Postoperative five-year survival rate was 73.5%, 64.1%, 34.9%, and 19.7% in HCC at BCLC stage 0, A, B, and C, respectively. The multivariate Cox regression analysis showed that HBV seropositivity, incomplete tumor capsule, vascular tumor thrombus, tumor diameter (≥3 cm), advanced BCLC stage (B+C), α-fetoprotein (≥20ng/ml), and direct bilirubin (>8µmol/L) contributed independently to shorter overall survival (OS); whereas post-operative radiofrequency ablation and second resection independently improved OS in HCC. HCV-HCC had a more favorable prognosis than did HBV-HCC (Log-rank test, P<0.001). A nomogram composed of age, gender, and the preoperative independent risk factors was accurate in predicting postoperative survival in HCC (C-index: 0.735; 95% confidence interval: 0.727-0.743).
Conclusion: HBV contributes to 84.4% of HCC in China, and actively promotes hepatocarcinogenesis and HCC progression. A favorable postoperative survival obtained in patients at the early BCLC stage highlights the importance of screening for early HCC in high-risk populations. Our preoperative prognosis prediction model is important in clinical decision-making.
Keywords: hepatitis B virus; hepatitis C virus; hepatocellular carcinoma; primary liver cancer; prognosis.
Copyright © 2022 Lin, Zhang, Yu, Bi, Zhang, Yin, Zhao, Liang, Qu, Wang, Hu, Liu, Wang, Zhou, Wang, Tan, Liu, Shao, Cai, Tang and Cao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Wang S, Du X, Han X, Yang F, Zhao J, Li H, et al. . Influence of Socioeconomic Events on Cause-Specific Mortality in Urban Shanghai, China, From 1974 to 2015: A Population-Based Longitudinal Study. CMAJ Can Med Assoc J = J l'Association medicale Can (2018) 190(39):E1153–e61. doi: 10.1503/cmaj.180272 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources