

Pneumonia Caused by Coinfection with Cytomegalovirus and Pneumocystis jirovecii in an HIV-Negative Infant Diagnosed by Metagenomic Next-Generation Sequencing
- PMID: 35800120
- PMCID: PMC9253620
- DOI: 10.2147/IDR.S364241
Pneumonia Caused by Coinfection with Cytomegalovirus and Pneumocystis jirovecii in an HIV-Negative Infant Diagnosed by Metagenomic Next-Generation Sequencing
Abstract
Background: Pneumonia produced by coinfection with Pneumocystis jirovecii (PJ) and cytomegalovirus (CMV) in infants and young children without timely diagnosis and treatment is often fatal due to the limitations of traditional tests. More accurate and rapid diagnostic methods for multiple infections are urgently needed.
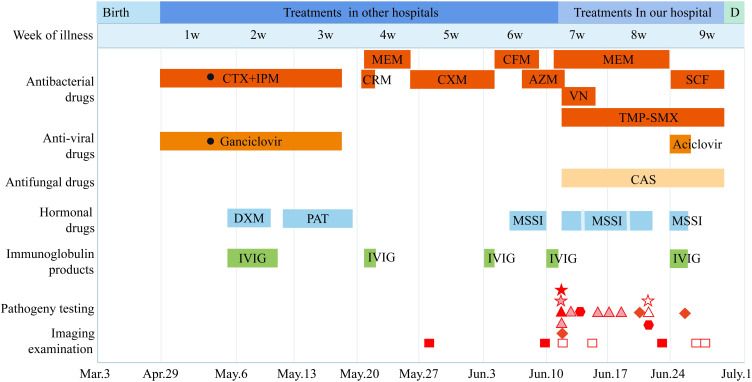
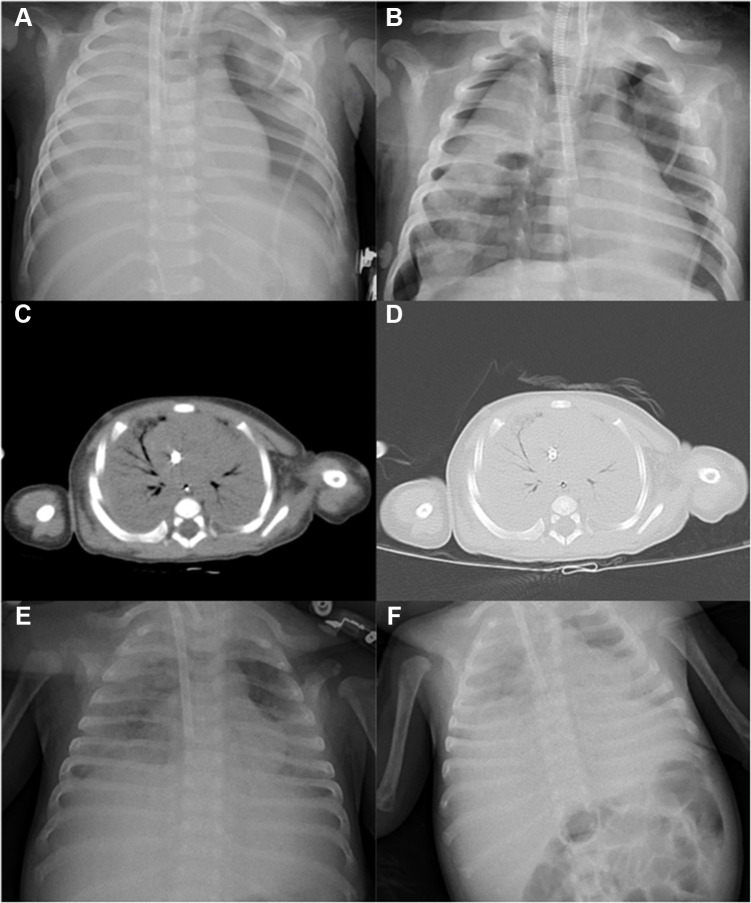
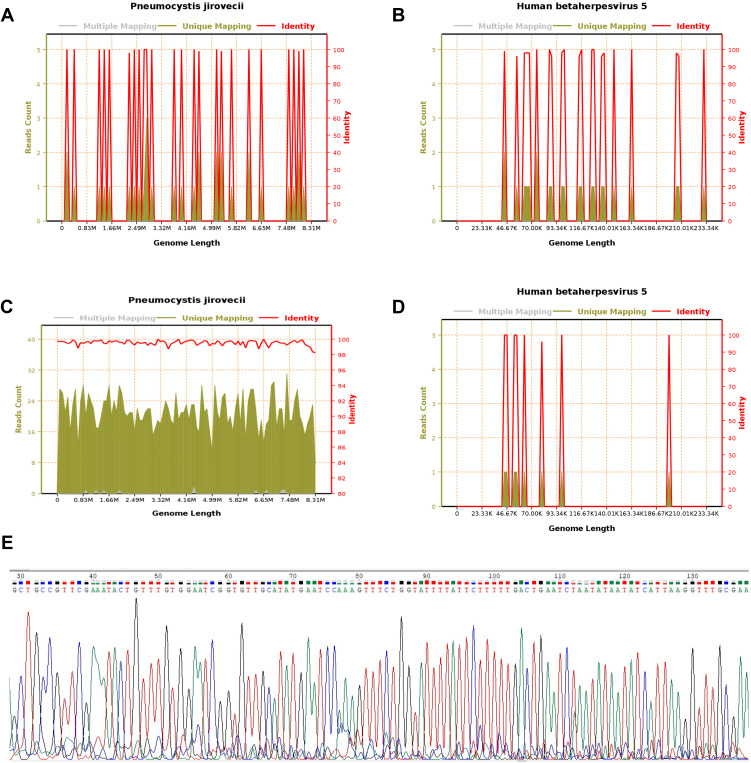
Case presentation: Here, we report a case of a 2-month-old boy with pneumonia caused by Pneumocystis jirovecii (PJ) and cytomegalovirus (CMV) without HIV infection. Chest computed tomography (CT) showed massive exudative consolidation in both lungs. Microscopic examination of stained sputum and smear specimens and bacterial and fungal culture tests were all negative, and CMV nucleic acid and antibody tests were positive. After a period of antiviral and anti-infective therapy, pulmonary inflammation was not relieved. Subsequently, sputum and venous blood samples were analysed by metagenomic next-generation sequencing (mNGS), and the sequences of PJ and CMV were acquired. The patient was finally diagnosed with pneumonia caused by PJ and CMV coinfection. Anti-fungal combined with anti-viral therapy was given immediately. mNGS re-examination of bronchoalveolar lavage fluid (BALF) also revealed the same primary pathogen. Therapy was stopped due to the request of the patient's guardian. Hence, the child was discharged from the hospital and eventually died.
Conclusion: This case emphasizes the combined use of mNGS and traditional tests in the clinical diagnosis of mixed lung infections in infants without HIV infection. mNGS is a new adjunctive diagnostic method that can rapidly discriminate multiple causes of pneumonia.
Keywords: HIV-negative; Pneumocystis jirovecii; cytomegalovirus; metagenomic next-generation sequencing; pneumonitis.
© 2022 Lyu et al.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Unusual Talaromyces marneffei and Pneumocystis jirovecii coinfection in a child with a STAT1 mutation: A case report and literature review.Front Immunol. 2023 Feb 20;14:1103184. doi: 10.3389/fimmu.2023.1103184. eCollection 2023. Front Immunol. 2023. PMID: 36891307 Free PMC article. Review.
-
Case Report: Next-Generation Sequencing in Diagnosis of Pneumonia Due to Pneumocystis jirovecii and Cytomegalovirus in a Patient With HIV Infection.Front Med (Lausanne). 2021 Mar 29;8:653294. doi: 10.3389/fmed.2021.653294. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33855038 Free PMC article.
-
Diagnostic Value of Bronchoalveolar Lavage Fluid Metagenomic Next-Generation Sequencing in Pneumocystis jirovecii Pneumonia in Non-HIV Immunosuppressed Patients.Front Cell Infect Microbiol. 2022 Apr 8;12:872813. doi: 10.3389/fcimb.2022.872813. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35463643 Free PMC article.
-
Metagenomic next-generation sequencing of bronchoalveolar lavage fluid from children with severe pneumonia in pediatric intensive care unit.Front Cell Infect Microbiol. 2023 Mar 16;13:1082925. doi: 10.3389/fcimb.2023.1082925. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37009495 Free PMC article.
-
X-linked hyper IgM syndrome with severe eosinophilia: a case report and review of the literature.BMC Pediatr. 2022 Apr 4;22(1):178. doi: 10.1186/s12887-022-03251-z. BMC Pediatr. 2022. PMID: 35379217 Free PMC article. Review.
Cited by
-
Unusual Talaromyces marneffei and Pneumocystis jirovecii coinfection in a child with a STAT1 mutation: A case report and literature review.Front Immunol. 2023 Feb 20;14:1103184. doi: 10.3389/fimmu.2023.1103184. eCollection 2023. Front Immunol. 2023. PMID: 36891307 Free PMC article. Review.
-
Diagnostic value of metagenomic next-generation sequencing using bronchoalveolar lavage fluid samples for pathogen detection in children with severe or refractory pneumonia.Microbiol Spectr. 2025 Mar 4;13(3):e0108724. doi: 10.1128/spectrum.01087-24. Epub 2025 Feb 4. Microbiol Spectr. 2025. PMID: 39902982 Free PMC article.
-
Pulmonary co-infections by Pneumocystis jirovecii and Herpesviridae: a seven-year retrospective study.Ann Clin Microbiol Antimicrob. 2024 Jan 20;23(1):8. doi: 10.1186/s12941-023-00663-2. Ann Clin Microbiol Antimicrob. 2024. PMID: 38245721 Free PMC article.
-
Clinical Features and Value of Tracheal Aspirate Metagenomic Next-Generation Sequencing for Severe Pneumonia in Children in Pediatric Intensive Care Unit.Pol J Microbiol. 2025 Jun 18;74(2):192-205. doi: 10.33073/pjm-2025-016. eCollection 2025 Jun 1. Pol J Microbiol. 2025. PMID: 40544519 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
