

Postoperative growth rate affects time to growth arrest after percutaneous physiodesis: A radiostereometric analysis
- PMID: 35800652
- PMCID: PMC9254027
- DOI: 10.1177/18632521221105781
Postoperative growth rate affects time to growth arrest after percutaneous physiodesis: A radiostereometric analysis
Abstract
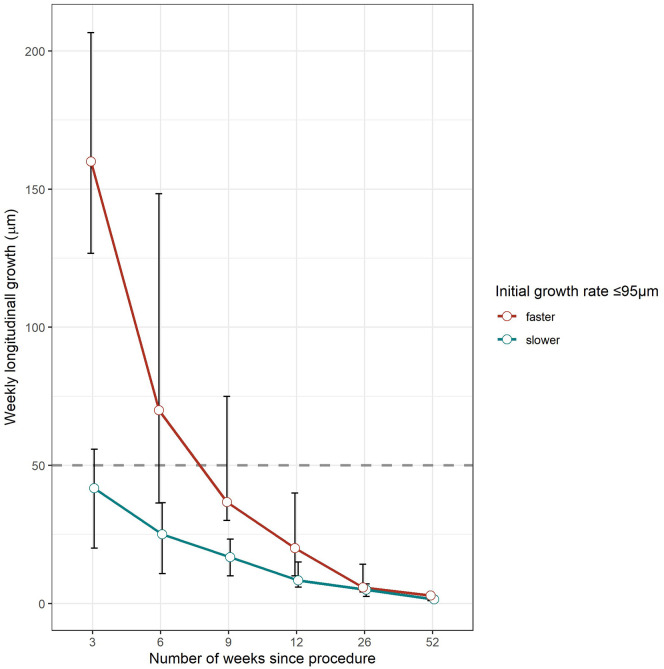
Purpose: The aim of this study was to determine the time at which physeal arrest is achieved after percutaneous physiodesis, and whether immediate postoperative growth rate affects the time to reach physeal arrest.
Methods: Radiostereometric analysis, with implantation of tantalum balls as radiographic markers on each side of the physes, was used to measure residual longitudinal growth in 21 children (10 boys and 11 girls) after percutaneous physiodesis for leg length discrepancy or extreme tall stature. In total, 25 femoral and 20 tibial physes were operated on. Median age at surgery was 13.9 years (range = 11.4-16.1). Radiostereometric analysis was performed postoperatively and after 3, 6, 9, 12, 26, and 52 weeks. Longitudinal growth rate <50 µm per week was defined as physeal arrest. Descriptive statistics were used for evaluation.
Results: Physeal arrest was obtained in 19 of the 21 children (40 physes) within 12 weeks postoperatively. One child was reoperated on in three out of four physes because of continued growth, and in one child, delayed physeal arrest was present at 26 weeks postoperatively. Time to physeal arrest was longer in physes with a higher immediate postoperative growth rate.
Conclusion: Postoperative follow-up with radiostereometric analysis at 12 and 15 weeks can determine whether physeal arrest has been achieved. The immediate postoperative growth rate after physiodesis seems to affect the time to physeal arrest. This implies that the risk for complications is greater for children during an accelerated growth period, for example, in boys, younger children and in distal femoral physes.
Level of evidence: level III.
Keywords: Percutaneous physiodesis; leg length discrepancy; physeal arrest; radiostereometric analysis; tall stature.
© The Author(s) 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures






References
-
- Scott AC, Urquhart BA, Cain TE. Percutaneous vs modified phemister epiphysiodesis of the lower extremity. Orthopedics 1996; 19(10): 857–861. - PubMed
-
- Kemnitz S, Moens P, Fabry G. Percutaneous epiphysiodesis for leg length discrepancy. J Pediatr Orthop B 2003; 12: 69–71. - PubMed
-
- Blair VP, 3rd, Walker SJ, Sheridan JJ, et al. Epiphysiodesis: a problem of timing. J Pediatr Orthop 1982; 2(3): 281–284. - PubMed
-
- Makarov MR, Dunn SH, Singer DE, et al. Complications associated with epiphysiodesis for management of leg length discrepancy. J Pediatr Orthop 2018; 38(7): 370–374. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
