

Multimodal Treatment of Hepatocellular Carcinoma in Patients With Hepatitis C Virus Infection Treated With Direct-Acting Antivirals
- PMID: 35800821
- PMCID: PMC9246468
- DOI: 10.7759/cureus.25487
Multimodal Treatment of Hepatocellular Carcinoma in Patients With Hepatitis C Virus Infection Treated With Direct-Acting Antivirals
Abstract
Background: Direct-acting antivirals (DAAs) opened a new era in the management of hepatitis C virus (HCV)-associated liver disease. However, hepatic cancer screening should not be stopped after obtaining a sustained virologic response (SVR). Current guidelines offer several treatment options for hepatocellular carcinoma (HCC), mainly depending on its stage and the extent of liver disease, including tumor resection, liver transplantation (LT), radiofrequency ablation (RFA), transarterial chemoembolization (TACE), and systemic agents. This article provides an overview of treatment modalities for hepatocellular carcinoma and associated survival rates based on the experience of the Internal Medicine Center at Fundeni Clinical Institute while bringing into light previous medical research.
Methods: We included 59 patients with a personal history of hepatitis C virus infection, diagnosed with hepatocellular carcinoma at least one year after achieving a sustained virologic response through direct-acting antivirals. The albumin-bilirubin (ALBI) score and Barcelona Clinic Liver Cancer (BCLC) classification were assessed in each case, and all patients were treated accordingly. The subjects were monitored by liver function tests, tumor markers, blood cell count, coagulation profile, and imaging explorations. We investigated the Eastern Cooperative Oncology Group (ECOG) performance status, the response to applied treatments, and survival.
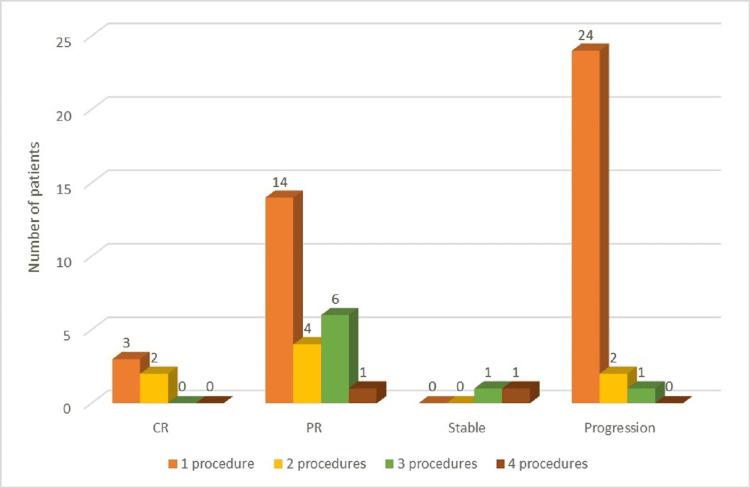
Results: Cirrhotic patients and multinodular tumor patterns were predominant. Most patients only experienced one therapeutic procedure, while the rest of the study group went through multiple treatment modalities (2-4), with a better outcome in terms of survival parameters. A large proportion presented with disease progression despite the therapeutic measures applied. A total of two liver transplants were performed, resulting in a 12-month disease-free period among these patients. The presence of diabetes mellitus (DM), multinodular disease, alpha-fetoprotein (AFP) over 300 ng/mL, and tumor dimension over 6 cm indicate poor overall survival. Both overall survival and progression-free survival were better in subjects who presented complete responses (CR) to HCC treatment. In patients undergoing a single intervention, the best overall survival was associated with surgical resection and RFA.
Conclusion: The multimodal treatment of hepatocellular carcinoma represents the best approach, in order to maintain patients on the waiting list for liver transplantation. In hepatitis C virus infection, viral clearance is important to obtain. At the same time, particular attention should be paid to liver cancer screening even after obtaining a sustained virologic response.
Keywords: direct-acting antivirals; hepatitis c virus infection; hepatocellular carcinoma; liver transplantation; sorafenib.
Copyright © 2022, Mercan-Stanciu et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures








References
-
- Geographical and temporal variation in the incidence and mortality of hepato-pancreato-biliary primary malignancies:1990-2017. Weaver AJ, Stafford R, Hale J, Denning D, Sanabria JR. J Surg Res. 2020;245:89–98. - PubMed
-
- Hepatocellular carcinoma. Villanueva A. N Engl J Med. 2019;380:1450–1462. - PubMed
-
- Hepatitis C virus associated hepatocellular carcinoma. Khatun M, Ray R, Ray RB. Adv Cancer Res. 2021;149:103–142. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous